Wikipedia has a good section on oral and maxillofacial pathology, with plenty of references to the literature if you want to explore mouth hard and soft tissue lesions more completely.
Organization of this Chapter
You May Skip to Whatever Subject Interests You Now
Basics
Bone Lesions
Lesions that ADD
Lesions that SUBTRACT
Soft Tissue Lesions
Pigmented Lesions
White Lesions
Injury
Problems with the Gingiva
Fistulations
Bottom Line
………………………………………………………………………………………………………………………….
Basics
A lesion is anything out of the ordinary – not normal tissue in a location where everything should be uniform and healthy.
There are lesions that involve the bone, and there are lesions that involve the gums and mucosa.
There are lesions that subtract from the local tissue, whether it be bone or soft tissue, and there are lesions that ADD to it – making the bone more dense or protruding, or that make soft bumps on the lining of the cheek, for example.
There are soft tissue lesions that are colored, and there are some that are white.
The upshot of all of this is that lesions are categorized in terms of these characteristics.
Bone Lesions
Lesions that ADD
One of the most common of these is called the torus. There are mandibular tori and palatal tori. You might have one of these already but are so used to it that it is not noticeable anymore. On the center of your palate there may be a hard bump – it could be small or large, but it is there. It is harmless, other than if you need a denture or partial denture that would cover the palate, the center of it needs to make room for the torus.
The mandibular torus can be felt along the inside edge of the jaw bone on the left or right. If you stick your tongue to either side near the floor of the mouth, if you feel a little protrusion from the jaw bone, that is it. Again, harmless unless you need to get a denture that covers the area. If the torus is large enough under these circumstances, you may need to have it surgically removed.
Possibly there will be growths of bone on the outside of the bony ridge as well, often bilaterally.
What causes these? That is uncertain, but in some instances it could have to do with excessive biting or grinding forces that are transmitted to the bone. The bone adds to itself to make it stronger to be more resistant to excessive force.

Lesions that SUBTRACT
Mostly these lesions are detected by X-ray or MRI or another imaging technique. They need to be distinguished from normal structures.
Normal Observations:
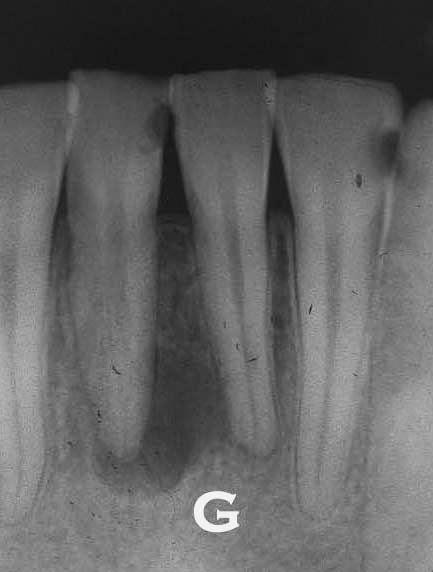
When you look at an X-ray there are various things that make the density of the bone locally lower – which will show up as a darker region on the X-ray. For example, the sinuses on the upper arch are hollow areas and some of them can be seen in most X-rays, and it is expected that they will be seen. The nasal cavity may show up in some X-rays. The passage of the mandibular nerve through the jaw from back to front may be seen as a darker line which represents the canal through which it passes. And, where this nerve sends a branch out through the bone near the lower premolars there is a FOSSA, a hole in the bone, through which this branch passes, that shows up as a dark circle in the X-ray. All of these darker areas are expected on the X-rays.
Abnormal Observations for Bone:
If there is a circular darker area centered on a root apex, it could be a cyst or abscess there as a result of infection in the tooth. Normally that will suggest root canal therapy. The X-ray needs to be taken from two different angles to get a 3-dimensional idea as to if it is actually AT the root tip or just behind it or in front of it.

If there is a circular darker area NOT associated with a root apex, particularly if centered on the midline of the mouth on either the upper or lower arch, it may be a cyst growing in the bone. I had one of these on the palate just behind the incisors and had it surgically removed. Cysts are completely benign, other than possible pressure they put on surrounding tissues. The pressure on the bone in this case will cause the bone cells to erode the bone to make room.
Irregular darker areas that show up in an X-ray may be more complex that described above. These tend to be rare, and a detailed discussion here is not appropriate, but irregular growths tend to be signs of serious problems. Both multiple myeloma and jaw osteomyelitis will show up in X-rays and possibly clinically as well – and both are serious, but fortunately, rare diseases.
Soft Tissue Lesions
Listed below will be brief descriptions of possible observations by category. It is important to note that there are over 300 dermatological diseases, and many of these can affect the mucosa of the mouth as well. We can only highlight here some of the more common or more worrisome.
Pigmented Lesions:
- Amalgam Tattoo – this is where some amalgam powder got trapped in the tissue during a restoration. It will stay there forever. A likely scenario is that a tooth was restored with amalgam, but the restoration had to extend under the gumline because of excessive decay. The amalgam got into the gum tissue there, and later, after the tooth was lost, it is still there making a dark pattern under the tissue.
- Nevus – this is basically a mole on the inside of the mouth. These are more unusual than those on the skin, but they are seen. There are a couple of different types, and they can either be flat or raised, and generally are not considered harmful at all. BUT – when you have pigmented lesions in the mouth, especially of recent origin, they should be checked to see if they are melanotic.
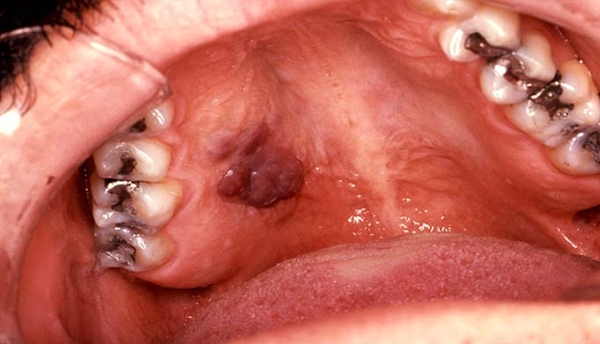
- Melanoma. This is a cancerous lesion which is quite serious, whether on the skin or on the oral mucosa. Wherever a melanoma is found, the problem is that it will metastasize – that it it will jump to other parts of the body. Whenever you have a pigmented lesion in the mouth, it should be biopsied to see if it is benign or malignant. If this pigmented lesion is irregular in shape with variation in color and in the area of 5 mm wide, it is suspect.
- Karposi’s Sarcoma – this type of cancer can exist in many locations in the body, but a pigmented lesion on the right or left sides of the posterior palate is sometimes the first sign of the disease. It has long been associated with HIV infection as a part of AIDS. Dentists are quite aware of the importance of any such observation, but few have ever seen it, fortunately.
- Unknown. The third picture below shows an image of a patient’s tongue that concerned me a lot when I first saw her. When I asked her about the discoloration, if she were aware of it, she said she had had it all her life, never changing in all that time. I have no idea what caused it, but the consistency and long-term existence ruled out anything that was a bad possibility.


White Lesions:
Again, there are MANY white lesions that can be observed in the mouth. Here will be listed just a few. If you search for any of these online, there are many places where much more detailed descriptions are given.
- Candidiasis, or thrush. This is a yeast infection of candidi albicans, and presents as a whitish layer over the tongue and cheeks. It is sometimes a complication of a compromised immune system, or extended use of antibiotics. This whitish layer can often be rubbed off leaving a red and bleeding area underneath. Your mouth will be sore and possibly burning. It can be treated by antifungal medications and is not considered a major health risk.
- Geographic Tongue

This looks painful but is not necessarily. And the origin of the name is easy to see, often they look like little maps of the world. It may involve some burning when eating spicy foods however. Oral rinses, perhaps involving steroids may be used, but this often just goes away on its own.
3. Lichen Planus – this may be confused with the two conditions above. It also is a pattern of whitish lines or patches on various soft tissues. It can be benign and go away on its own, or it can progress to an ulcerative condition which will need careful management. Oral steroid creams can be helpful, but the cause is generally not known.
4. Apthous Ulcers – otherwise known as CANKER SORES. Some people are plagues by these things and some people have never had one. I used to get them a lot in my earlier decades. While the cause is not certain, the stimulus for them can be as simple as biting your lip. I associated them with some kind of cut in the mouth when eating a lot of sugar. These things HURT. They tend to last on their own for 7 – 10 days, and eating can be painful for this whole time. There is a medication called Kenalog in Oragel, which is a steroid in a gel that coats the ulcer and heals it much faster – in a couple of days. Simple over the counter medications tend to be gels or pastes that cover the sensitive areas on the borders of the ulcer, and perhaps an added anesthetic like benzocaine. They are called DENTURE SORES when they arise under the border of a denture that does not fit well and irritates the mucosa. For denture sores the Kenalog product is great. There is some more discussion on this topic in Chapter IV.1 in the discussion of pain.

5. Ulcers that are painless – this is a problem. If it LOOKS like a canker sore, but doesn’t hurt, your dentist will arrange to have it biopsied immediately, because painless ulcers are a sign of cancer.
6. Smokeless Tobacco lesions – these are whitish areas around where the tobacco product or snuff is placed. Of course the baseball industry has seen a LOT of this over the decades. While it is suggestive that if tobacco causes cancer in the lungs it might in the mouth as well, but I have seen no evidence of this being the case. Just the appearance of the lesion is scary, however, and it is certainly recommended that one discontinues the practice.
7. Aspirin burns. These generally occur when someone finds relief from a toothache by placing an aspirin tablet in the mouth against the mucosa near where the tooth hurts. It is a harmless white area of damage caused by the aspirin, but the main problem is not that – it is the tooth!
8. Herpetic gingivostomatitis. This is a herpes simplex type 1 virus infection of the mouth. It may be even in childhood that the infection occurs by exposure to someone with the virus, and children will have ulcers or bumps and soreness with a fever for a while – but the virus stays in the body forever. After this initial infection the typical presentation is as HERPES LABIALIS – COLD SORES on the outside border of the lips. The type 1 infection is different from the type 2, which is more responsible for genital herpes. It is rare that type 2 will infect the mouth, but it can happen.

9. Verruca Vulgaris – this is basically a WART inside the mouth – and presents the same way as on the skin. It is an infection of the human papilloma virus, HPV. These are benign lesions which can stay in place without issue, or can go away on their own. If one grows in a place where it is subject to being BITTEN, it is a good idea to have it removed.

Injury
- Cheek biting – generally seen at the back of the mouth. If the relationship between the opposing teeth does not place the upper tooth sufficiently extended beyond the position of the lower tooth, the upper tooth does not push the cheek aside as the teeth bit together. This may lead to a situation where frequent cheek biting is experienced. Other than the pain involved at the time, there may be an extension of the soft tissue that forms (making it even EASIER to bite), and a canker sore could form in the traumatized area as well. Typically it only happens a couple of times and when it you bite down while distracted by something in the environment. But if it happens a lot, see your dentist about changing the contours of the teeth in that area.
- Mucocele. These are also due to trauma, and often on the lips due to biting or being hit in the mouth. It is a swelling which may be skin colored or bluish that is filled with fluid, often salivary fluid. If the lip was damaged so that the saliva cannot get out of its duct, then the swelling results. Often they will go away without treatment.
- Fibroma – when recurrent trauma is happening it is possible that a fibroma will occur in that location. It may be on the tip of the tongue as an example. It is probably the same color of the surrounding tissues, but elevated. It can be whitish as well. It may be considered scar-like in nature, but as the name implies, it is the fibrocytes, those cells that make the fibrous connective tissues in the area, that are overworking. They may well involve no symptoms, but if persistent biting is occurring in that location, the chances of biting the fibroma are high. Surgical removal is a simple procedure, and the occlusal relationship of the opposing teeth should be investigated by the dentist.


Problems with the Gingiva:
- ANUG – also called Trench Mouth or Acute Necrotizing Ulcerative Gingivitis. That sounds horrible, I know. Poor oral hygiene and smoking are predisposing factors, and it can come on quickly, but it is painful. It is the result of an infection of a particular bacterium, and can be managed by antibiotics and potentially removal of dead tissue if any has formed by trying to ignore the condition. The name, trench mouth, comes from the soldiers in the trenches of World War I, who developed this disease frequently due to the limited possibilities of oral care. When I was in college there was a fellow student that I knew that developed this condition. That is the only case I have seen, but I know he was miserable. After that his nickname became “Trench” – so best to keep up your home care if you don’t want that nickname.
- Gingival hyperplasia – this can be a tremendous overgrowth of the gingival tissue – without much additional coloring. When the gingival tissues cover much of the facial surfaces of the teeth, there is something very wrong. In most cases this has been the direct result of one particular drug used for epilepsy – dilantin. But there are several classes of drugs that cause this condition. Whatever you may be taking in terms of medications, check the side effects. If they have oral side effects, at least make sure you are doing great home care.
Fistulations
This is not a disease state of the soft tissues, but is the result of infection in other tissues of the mouth – typically from abscesses either at the apex of tooth roots, or in the periodontal pockets. If an abscess occurs, it involves the production of “pus” or an exudate which consists of dead cells and products from the immune reaction to the infection. This material must GO somewhere, and sometimes that is THROUGH the tissue. There will be a little HOLE in the tissue through which passes this material.
Two things – first the TASTE of that material is not at all pleasant, and the smell of your mouth will be unpleasant – second, we can follow the channel back through this hole to see where the infection is located.
Often the dentist can take a gutta percha point, used for filling root canals and somewhat opaque to the X-ray beam, and insert it through the hole and use the X-ray to see where it goes. It may well lead directly to the apex of a tooth that is infected. The good news is that when the tooth is treated with root canal therapy, the infection will go away and the bone will regrow and the fistulation will fill in.
Bottom Line for Mouth Hard and Soft Tissue Lesions
This is just the tip of the iceberg when it comes to hard and soft tissue oral lesions. I’ve mentioned some of the most common, but also some of the ones you want to really watch out for.
There are MANY systemic disease states that will produce some symptoms in the mouth. Sometimes this is a GOOD thing, because the dentist can make an observation that tells him that you may have this particular disease, and it may be the earliest sign of this disease. When a disease is identified early, there is a better chance of curing it.
So, one of the important reasons for making regular dental appointments is for the dentist to have the opportunity to check your mouth carefully, not just the teeth, to see if there is anything that is showing up that might portend something more serious.