Crooked teeth and malalignment result in malocclusion – and this subject is covered well on Wikipedia with references to the literature if you want to get into this in more detail.
Organization of this Chapter
You May Skip to Whatever Subject Interests You Now
Basics
The Nature of the Problem
Causes of Malocclusion and Malorientation
Genetics
Decay in Primary Teeth
Decay in Permanent Teeth
Bad Habits
Prevention
Treatments
Bottom Line for Crooked Teeth
……………………………………………………………………………………………………………………..
Basics
In this chapter we’ll take a look at various classifications of abnormalities in orientation of single and multiple teeth relative to other teeth or to the bone – in other words crooked teeth.
The causes of irregular positioning and orientation, the prevention of further changes in tooth orientation, and the treatments all need to be discussed.
The general dentist will have a pretty good idea what is going on in your mouth in this area, but will typically not do the work themselves. You will often be referred to an orthodontist, especially when the ensuing problems can be seen at a young age.
Or, you could be referred to an orthodontist as an adult, to correct malalignment problems that you feel are cosmetically significant.
Or – the general dentist may choose to make orthodontic changes themselves using repositioning appliances, for example the InvisAlign system. Visit Chapter V.17 for more discussion of the possibilities here.
Crooked Teeth: The Nature of the Problem
Problems in alignment can happen because of the basic boney structure in the mouth – basically because of original equipment – OR because of changes that happen as things happen historically in the mouth.
The dental arches should, ideally, have every tooth fitting into its designated location and having its appropriate size, and the upper and lower arches should match. In the real world this rarely happens. Dentists have three classifications or arch relationships, based on whether the upper arch is in normal position relative to the lower (Class I), whether it is positioned ahead of the lower (Class II), or whether the lower arch is ahead (protrusive) relative to the upper (Class III). It happens that ethnic groups have different tendencies to have certain classes, for example Class III is very common for the Japanese, whereas Class II is more common in the U.S. Class II and Class III deviations can lead to particular bite problems, especially later in life, but neither is necessarily critical as long as the appearance is acceptable and the upper and lower teeth have a fairly even and well supported occlusal scheme (the upper and lower teeth stabilize each other in biting).
A similar consideration that is useful is based on the amount and nature of overlap between the upper and lower teeth. You should be aware that the upper teeth are supposed to lie OUTSIDE the lower teeth when you are biting down. Obviously the upper front teeth hang over the lower teeth in most people, (except extreme Class III individuals), but the same is true normally for the back teeth as well. If there is a deviation in part or all of the arch, where the facial cusp of the upper tooth occludes with the groove of a lower teeth, this is called CROSSBITE.
The following picture shows an illustration of crossbite where several teeth are involved. Where single teeth are in crossbite, it is usually due to a lower tooth being tipped to the outside, or an upper tooth being tipped to the inside (toward the palate). When more of the arch is involved it is usually because the upper arch is too small for the size of the lower arch.

Another type of bite that is commonly observed and can have very bad effects later in life is the OPEN BITE. In this situation the back teeth close together, more-or-less normally, but in this biting position there is still a large space between the upper and lower front teeth. Sometimes there is no occlusion except at the molars. Generally this scheme will result in a great deal of wear on the occluding teeth, and it is difficult to fix without surgical procedures where the bone that holds the upper teeth is cut apart and repositioned.
We’ve all seen people that have teeth that are way out of the normal alignment of the rest of the teeth. Most often this affects the canines, where they are the last teeth to come into the arch and they have found no room. This is called BLOCKED-OUT CANINES, and has very specific causes, involving the degree to which the primary teeth were cared for.
It must be noticed that all of the above situations describe problems with the way the teeth erupt originally. Now we must also consider changes that as we age and our dental situation alters, things CHANGE in the mouth. In other words, our tooth alignment can change with HISTORY.
For example – as teeth are LOST, other teeth move to fill the space, and this will throw off the alignment of, potentially, the whole arch of teeth. Problems with the Primary teeth will affect their positions and the permanent teeth will come in wrong because they are not guided properly. And, problems with the Permanent teeth can cause them to shift after eruption – possibly much later in life.
Let us now turn to further description of the cause of some of these problems, followed by a look at preventive and corrective measures.
Crooked Teeth: Causes of Dental Malocclusion and Malorientation or Malalignment
There are three kinds of causes for crooked teeth. The first is something over which we have no control, we cannot choose our parents and our genetic inheritance. The second cause relates to the care we take of our children’s primary teeth. The third relates to how we take care of our permanent teeth.
………. Genetic Problems
When your two parents have very different jaw sizes and tooth sizes, you can expect trouble. If your father is larger and you get his upper arch then a pronounced Class II dentition is expected. If you get your mother’s upper arch then you could “inherit” a full arch of crossbite. Often these arch discrepancies reveal themselves even before the primary teeth are lost, and often something can be done at that early date, as early as 6-8 years old.
Other than full arch discrepancies, you may have genetic mis-match that, within one arch, leads to problems. Even if your primary teeth seem to fit well together, there is often not enough room in the bone for all of the permanent teeth. If the length of the ridge is shorter than the widths of the teeth added together, then problems will result, most often short-changing the last tooth to erupt in the arch, generally the canine. It is also common to find that there is not enough room in the arch for the wisdom teeth (third molars), and sometimes even the second molars would have trouble fitting in.
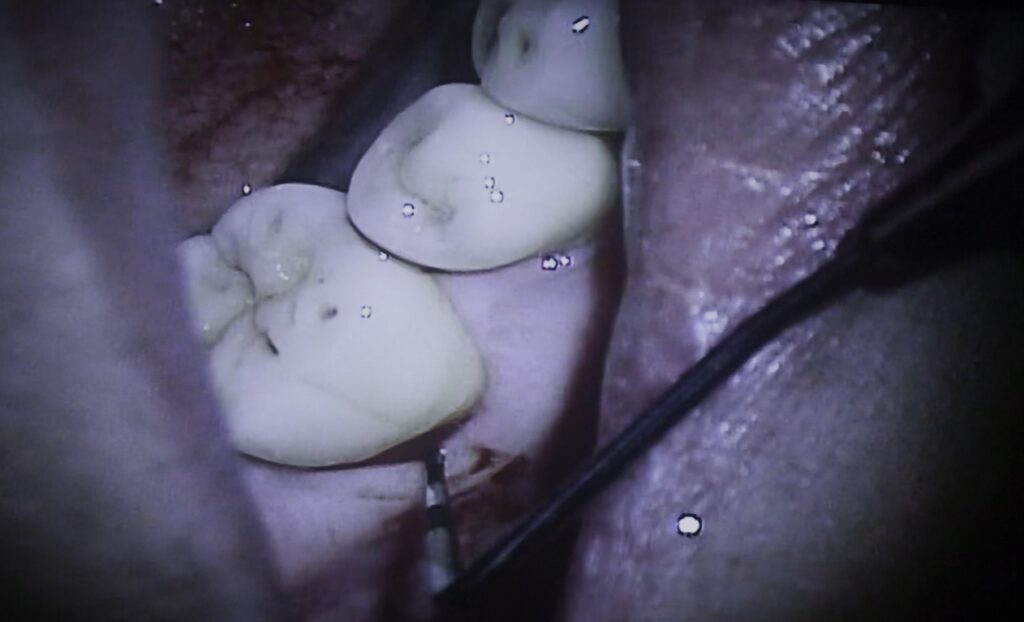
But, there also could be a little MORE room in the arch than is needed for the teeth. In this case there are sometimes spaces left in the front teeth, gaps called Diastema by dentists. There could also be enough room for teeth to erupt in various orientations – as seen in the picture above.
While a genetic predisposition toward malocclusion and malorientation is not avoidable, if recognized early enough it is correctable or at the very least you can take care not to make things any worse.
………. Decay Problems with the Primary Teeth, and Consequences
The primary teeth are absolutely vital for the determination of the alignment and occlusion of the permanent teeth. Obviously, genetic defects as described above can make things difficult under the best of circumstances, but even a genetically perfect dentition can be wrecked by not taking care of the primary teeth.
The primary teeth function as PLACE HOLDERS, or guides, for the permanent teeth as they form and erupt. Each primary tooth has a permanent tooth that will come up underneath it. And when the child is around six years old the first molars will come in BEHIND the primary teeth. What happens if the primary teeth are not there at all? Then the first molars will not have anything to guide them in and will erupt much closer to the front of the mouth than desired. Once the first molars are in, then the remaining space for the rest of the permanent teeth (10 more teeth in each arch) is SET. If the first molars come in even a few millimeters too far forward, then serious crowding could result.
It is easy to picture the scenario described above, where there are no primary teeth, or the last ones in the arch are missing, but essentially the same thing can happen when ANY primary tooth is missing or damaged in any way. The most frequent cause of damage to primary teeth, or of missing primary teeth is decay.
All too frequently we see kids that have such deep decay in their primary teeth that it affects the areas between adjacent teeth. In this case the neighboring tooth can actually lean forward into the decayed area. The damage that decay causes removes the hard tissue that is expected to support the adjacent tooth. If the decay is repaired early enough then a filling can be placed that will keep the tooth behind it from leaning in any more, and prevent shortening the arch and crowding more than genetically determined.
But what if the decay on a primary tooth is too advanced to save the tooth and it must be extracted prematurely? Now we have a major space problem, where the teeth erupting behind this space can be expected to lean into it, closing the arch and leading to a blocking-out of the permanent canines (at least).
The appeal must be made to monitor the primary teeth of your children very carefully to see that this doesn’t happen. It’s all too common that a few years of inattention on the part of the parents doom the child to a really messy bunch of teeth and years of difficult orthodontics (if the parents can afford it). In a world where it’s hard enough to make the grade with everything going for you, then we saddle a child with a poor self-image to make things more difficult?
Visit Chapter V.19 for more on Dentistry for Kids.
………. Decay Problems with Permanent Teeth
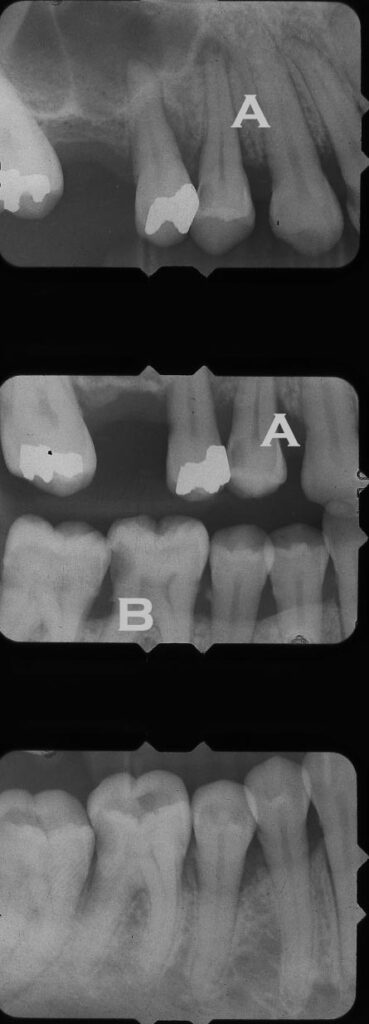
There are a variety of problems in the above X-rays that illustrate thesse concerns for the permanent teeth. In the area of “A” the relationship between the two premolars does not seem normally aligned and there is a space between the first premolar and the canine. The missing first molar may allow this movement. Taking into account the limited bone level, there is not much bone to maintain the teeth in one place. And, the relationship to the opposing teeth may push the upper premolars in unexpected directions.
In the case above, the missing tooth on the upper arch could have been caused by decay, but the consequences keep coming. The molar that opposes the missing upper tooth is erupting farther because there is no tooth biting on it. When it erupted farther, the contact with the second molar shifted toward the CEJ, and made the tooth more susceptible to decay.
And – the supereruption of the lower first molar AND the tipping movement of the first and second molars toward each other, allowed by the soft decayed area, have made more room for the lower premolars to shift and align poorly.
All of these observations in this case could have been triggered by the loss of the upper first molar, combined with limited bone support.
………. Bad Habits
Every known an eight year old child that still sucks their thumb?
How about someone who speaks with a tongue thrust, so the “s”‘s are kind of smashed up. Then there’s always studying with a pencil in your mouth, prying the teeth apart for hour after hour each day. All of these things can really mess up your teeth, generally flaring the front teeth way out, pushing the lip forward and making for a pronounced “beaver” appearance.
The tongue thrust can cause an open bite in the front. Can you imagine spending $25,000 on a surgical procedure to close the bite, let alone six weeks with your mouth wired shut, only to have the teeth move right back the way they were with a few months of tongue thrusting!
Thumb sucking for the young kids is O.K. But after the age of 5 or 6 one want to work hard to keep those permanent teeth coming in straight. There is an appliance that is cemented to the teeth which holds a wire around the inside of the upper front teeth. This wire has soldered to it lots of little sharp pokey things which really hurt when you catch your thumb on them! Sounds like an intra-oral Spanish Inquisition doesn’t it? But, it works, and most kids do well with it. I don’t see how that’s possible, but they do! It does wonders for a tongue thrust problem too!
Crooked teeth: Prevention
The major preventive measure you can take are to pick your genes carefully from your parents gene pool and to avoid any decay in your primary teeth. Obviously we can’t do the former, but if you have a decay problem then do not delay getting to the dentist and having it fixed! Now you know one of the major reasons for making sure that this is done.
There are other corrective measures that can be called preventive. When it is determined that the upper arch is too small, arch expansion devices can be used to actually spread the bones apart a little more and widen the palate. These devices are attached to the teeth (first molar particularly) or can be removable. This procedure will prevent many of the bone mismatch problems that would otherwise have occurred.
One thing to look for in kids is space between their primary teeth, particularly in the front of the mouth. Some parents are concerned that there are spaces when for adults this is not considered esthetic or natural. For kids it is natural and much to be preferred. If these spaces are there and you can avoid decay in their teeth, then you have a good chance of achieving the best possible alignment of the teeth, given the genetic conditions. If there is no space between the front teeth then it would be a good idea to go to your dentist and have him/her do a consultation to see if there is anything that should be done early on.
Crooked Teeth: Treatments
We have already discussed one treatment, where the palate is widened in order to avoid full arch crossbite in the adult dentition. This type of treatment is really preparative for full orthodontic repositioning, which will be discussed more in Chapter V.17. Naturally, once the teeth are out of position, they have to be pulled or pushed back using some kind of mechanical contrivance. When there is no room into which the teeth can be moved, then extractions must be done. Sometimes one premolar is taken out both right and left, and sometimes top and bottom as well to provide the extra space.
But what about the rest of us? There are lots of people who have teeth that are not dramatically out of alignment, but as they get older they feel more sensitive to their physical appearance, and want everything to be nice and straight. Orthodontics for adults is certainly becoming more common these days. The new non-metal brackets, or even metal brackets for the front that don’t use wide metal bands all around the tooth, eliminate much of the reflective look of braces back in the “old days”. Braces for adults in a professional business environment are becoming much more acceptable.
But there are some who will not go through the long-term and time consuming orthodontic treatment, but they still want their teeth straight, at least the ones in the front. There are other alternatives, each of which will be discussed more in Chapter V.18 on Cosmetic Dentistry. Here we will only mention that the shapes of the individual teeth can often be altered in order to make them look like they are lined up more precisely. This can be done using plastic bonding, porcelain veneers, or even full crown placement for the most aggressive treatment. We are generally not treating FUNCTIONAL problems with these approaches, however.
There are times when limited orthodontic treatment, where only a few teeth have to be involved, is appropriate. This may be for cosmetic reasons, or because there is a molar which has tipped over and must be straightened up in order to use it to support a bridge or some other restorative appliance.
In the last decade a totally wireless approach to limited tooth movement has become marketed highly, Invisalign. This approach uses a succession of clear plastic positioners to gradually move the teeth – more by tipping than by bodily movement – but it can be effective in certain circumstances. More will be said about this in the Cosmetic Dentistry chapter as well.
Crooked Teeth: The Bottom Line
Teeth that appear crooked and abnormal in alignment can represent a social or even professional stigma.
When we are young, even before the permanent teeth fully erupt, the X-rays will show problems with the way the permanent teeth in the bone are aligned FOR eruption.
There are certain genetic predispositions that we can potentially correct, when done early enough.
Once the primary teeth have erupted, they must be cared for so that they provide the correct guidance for the permanent teeth to erupt normally.
Once the permanent teeth are in place, whether ideal or not, we need to care for them so that there will be no alignment changes because teeth are lost or damaged.