Dentistry for Kids is called pediatric dentistry, and the dentists who specialize in this area are pedodontists. They are some of the most empathetic people I’ve ever met!
The American Academy of Pediatric Dentists has a website that reflects this caring.
Wikipedia also provides references to the primary literature and description of what dentistry for kids is all about.
Organization of this Chapter
You May Skip to Whatever Subject Interests You Now
Pediatric Dentists
The Needle!
Nitrous – Laughing Gas and other sedation
Problems with Kid’s Teeth
Sealants
Deeper Decay
Space Maintenance
Alignment and Eruption Anatomy
Really Young Kids with Lots of Decay
Genetic Problems
Bottom Line for Pediatric Dentistry
…………………………………………………………………………………………………………………………….
Dentistry for Kids: Pediatric Dentists
I have known several dentists that specialize in working with children, and my hat is definitely OFF to them! First, they tend to be really great people – kind and gentle of nature, and always empathetic toward what the kids are going through. Second, they ENJOY working with kids, because that is who they are.
In my practice I worked with kids down to 5 years old – that was my lower limit. For kids younger than that it takes a more special talent that I possess, and I would generally refer these kids to my favorite pedodontists.
Dentistry for Kids: The Needle!
We are taught in dental school to never let the kid SEE the needle. Just sneak it in under the chair and into the mouth outside their peripheral vision even. This usually works pretty well. And, of course, the area where the needle penetrates is numbed with topical gel before hand.
When I was a student I had a 5 year old girl patient that had a really surprising propensity. I don’t know what her previous experiences were like with other dentists, but possibly bad and that is why Mom brought her to the dental school for treatment.
But, I would go through everything as normal, topical and sneaky. But, as soon as she felt the slightest pressure on the tissue from the needle, she JUMPED! And I mean high! Her butt would end up on the head rest and her head would be hanging backwards over toward my knees. Mom always sat right there reading and after a few visits like that she never seemed to notice. I developed the trick of following her head downward with the needle still (very well anchored to her head) in her mouth, and then I would grab her head between my knees and do the injection. After that, everything was fine!
I recall one time when a group of third year students was taking a tour of the pedo clinic just when I was doing an injection on this little girl and they saw the whole thing! I have never seen so many scared, wide eyed individuals in one place before or since ….
Nitrous and other Sedation
Laughing gas, or nitrous oxide, is a very useful adjunct for working with tense kids – it will calm them down and make it so that any discomfort doesn’t seem to bother them so much. I sometimes use it MYSELF in my dentist’s office if I want to enjoy an unenjoyable experience more.
When used at the correct concentrations mixed in with oxygen, it is something that most people should consider. There will be an extra charge for it, but for kids it may help them have a better experience and remember it more favorably for next time, because they will remember little of it.
Other kinds of SEDATION may be used in various situations, especially when working with rampant decay on a 2-year-old. This is normally done in a hospital setting. It WAS the case that some dentists that could not handle kids would use chloral hydrate (“knock out drops”) with small kids to sedate them so the dentistry could be done. This is inherently dangerous, and is not a current practice. But, I once met a dentist who had asked his assistant to administer chloral hydrate to a 4-year-old girl, and the poorly trained assistant administered TEN TIMES the allowed dose.
It still pains me to realize that such a monumental but simple mistake in a dental practice could cost the life of a patient – but it did.
Dentistry for Kids: Problems with Kid’s Teeth
Clearly the most common is decay. Kids to get decay often and the treatment can be anything from a sealant, to a filling, to extraction of the tooth.
Sealants
This is basically a thin composite material that will bond to the etched enamel of the tooth. The dentist may detect some areas that look decalcified, in the grooves and pits of the occlusal surface of the tooth. They may take a very thin bur and open up the grooves a little, to confirm that the decay or decalcification does not extend to the dentin, and then after etching the tooth the composite will flow into the area and be light cured.
It is not as likely to seal primary teeth, for they often will leave on their own (exfoliate) before long and a simple filling, while more aggressive, is possibly more appropriate. When the child is 6 or over, the first molars have erupted behind the 10 primary teeth in each arch, and these may well start to develop some decay, which a sealant may well arrest for many years.
Deeper Decay
When the decay gets deeper into the tooth a larger filling will be necessary, or possibly the pulp will be opened up and a pulpotomy will be done. This is not a root canal treatment, as the canals are not accessed. They may well not be accessed because the roots are resorbing under the pressure of the permanent tooth erupting below it anyway. But doing a pulpotomy and placing a stainless steel crown is a pretty common procedure.
The stainless steel crown is often needed, because if there is enough decay to expose the pulp, likely the sides of the tooth that are in contact with the adjacent tooth are involved as well, and the adjacent teeth can tip toward each other. If this happens, the space allocated for the erupting permanent teeth will be too small.
A stainless steel crown is a preformed shape of thin steel that looks like a tooth crown, but is contoured inward toward the gumline area. The tooth is cut down to allow the crown to “snap” over the tooth, and with some cement, it will protect the tooth and the space until the tooth is no longer needed.
Dentistry for Kids: Space Maintenance
This is one of the BIG issues with kids teeth – for if they loose a tooth or teeth, we still MUST maintain the space where the teeth were for the erupting permanent tooth.
The primary molars lie over the permanent premolars, and if the space is not there for the premolars when they are ready to erupt, they will move into the wrong place, or certainly cause the canine, which erupts later, to come in totally out of the arch.
When a tooth is extracted by a dentist or pedodontist, they will form a SPACE MAINTAINER. This cemented appliance will consist of a band which goes around a tooth adjacent to the space, with a loop of wire soldered to it which will push against the tooth on the other side of the open space. That way the teeth CANNOT mover toward each other.
There are space maintainers of various designs, and some cross over the midline to keep space on both sides of the arch, if other teeth are missing.
But the goal is always to make sure there is room available for normal eruption and bite of the permanent teeth.
Alignment and Eruption Anatomy
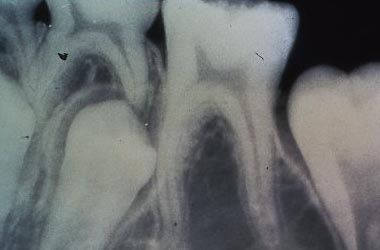
In the X-ray above you can see the permanent second premolar heading in the wrong direction. It should be coming in directly below the primary second molar, which you can see with an empty area between the roots. But, for some reason the premolar has other ideas.
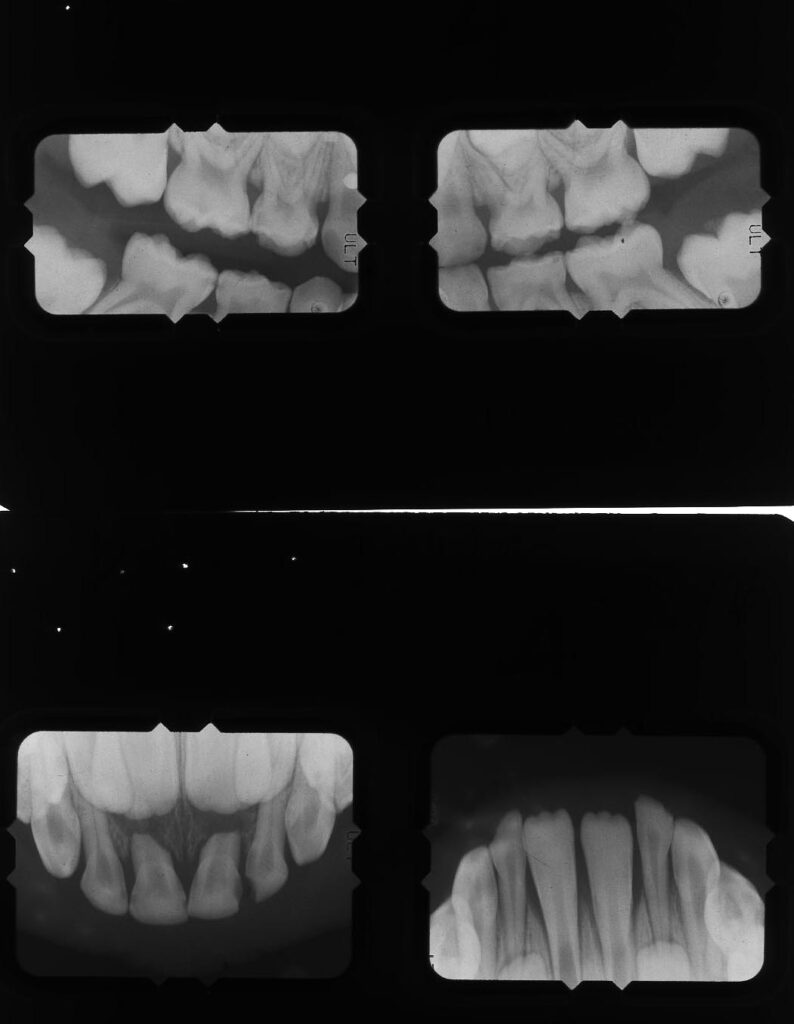
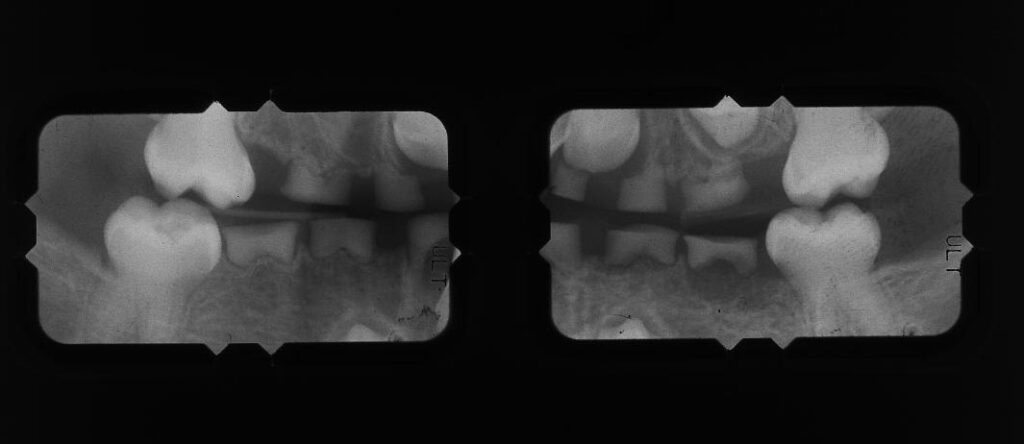
The X-ray above shows a fairly normal eruption pattern for the permanent teeth, as far as we can see from the anterior views at the bottom. The alignment of the upper central incisors seems symmetrical and the primary roots are resorbing uniformly. For the lower arch the permanent central incisors are already mostly in, and the laterals are seen below, but symmetrically disposed and looking normal.
For the upper X-ray above you can see that all of the permanent first molars are coming in behind the primary molars in the expected way.
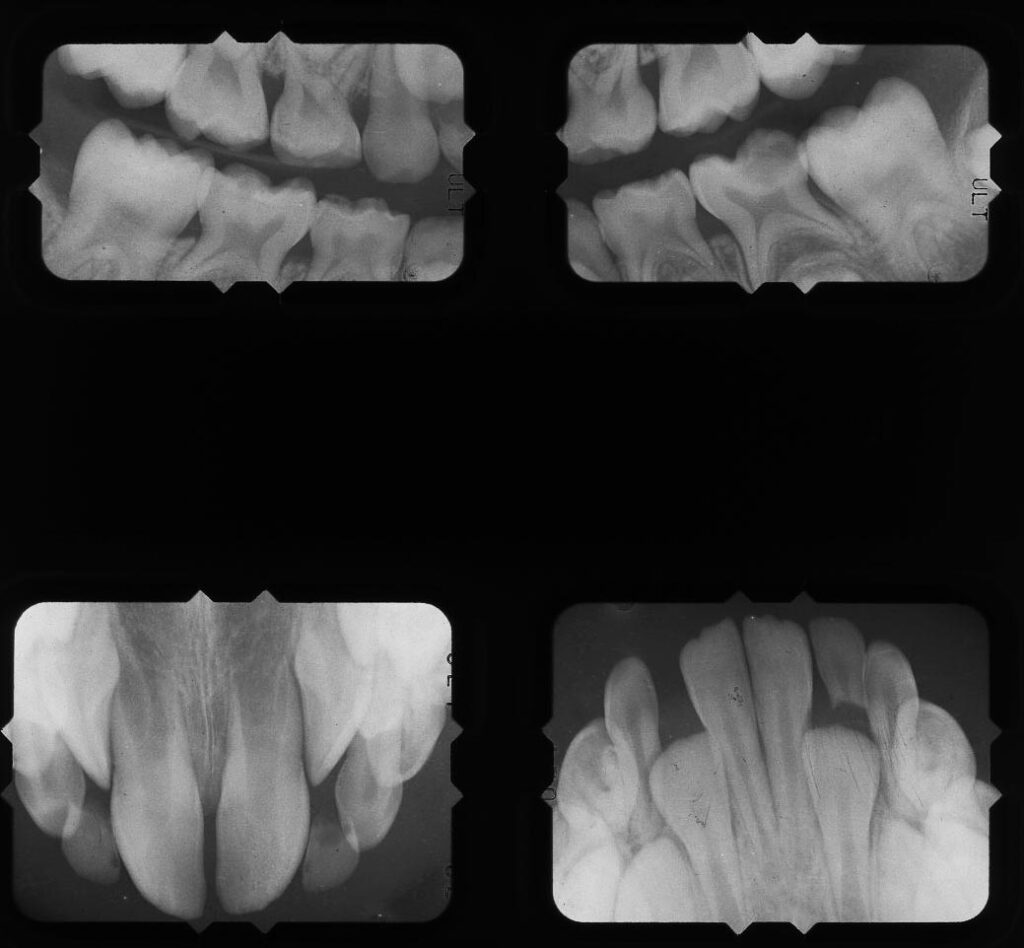
The X-ray above shows more problems with alignment and eruption. While the permanent molars seem to be coming in fine, the anteriors show signs of crowding. The upper central incisors are twisted and the laterals look like they, too, are rotating to fit into the available space. For the lower arch the centrals are in and the laterals seem symmetrically disposed. Both of the primary canines are still there and the roots have not started resorbing yet.

The picture above shows an appliance that can be made for a kid who has one permanent central that is coming in tilted to the lingual. This appliance sits on the other teeth and has a little spring that pushes on the central in question.
Really Young Kids with Lots of Decay
This is one of the things you read about in “baby books”. Parents are supposed to make sure that if their kid is taking nourishment from a bottle, that the bottle is not allowed to be IN the mouth for any significant length of time. Some parents just stick the bottle in and go about their business – even letting the kid fall asleep with the bottle there. The baby may use the bottle like a pacifier, every so often chewing on it, and a little milk comes out into the baby’s mouth. This formula may have sugar in it. READ the labels!

When the formula is constantly bathing the baby’s newly erupted primary teeth, it sets up the ideal condition for decay – and “bottle mouth” happens. I’ve seen 2 year olds with decalcification and decay on virtually every tooth in the mouth.
How do we handle this for the baby? We cannot expect them to sit in a dental chair and undergo that kind of traumatic treatment. It may require extractions, space maintainers, pulpotomies and stainless steel crowns, or even covering anterior teeth with preformed plastic crowns that are cemented over the teeth after decay removal and cutting down for the crown of the tooth.
In general, the pedodontist will have hospital privileges for this kind of procedure. The baby will be anesthetized and sedated so that the work can be done without any awareness at all. Of course, this is VERY expensive, but critical if the baby is allowed to get into that condition.
“Bottle mouth” has also been observed when women breast feed their baby and allow them to just hang on for long periods of time. Best to get the feeding done, rinse out the mouth, even brush the teeth with a fluoride paste and the baby is protected.
Genetic Problems
This is not such a common problem or typical in any way. But potentially devastating for the child if they inherit certain traits from the parents.
I had a family in my practice where the mother had lost all of her teeth at the age of 17, and had been wearing dentures since then, and she was 29 when I met her. Her oldest child was a girl that had normal teeth, but both boys, aged 8 and 5, had the same problem as the mother.
The disease that they had is called dentinogenesis imperfecta. Which basically means that the tooth doesn’t form well. In fact it is the junction of the enamel and dentin that does not form well. Apart from that, there is little or no pulp chamber or root canal system, but the major problem is with the enamel connection.
As the primary teeth erupt the enamel falls off and only the dentin is left, which is promptly ground down to the level of the gum line.
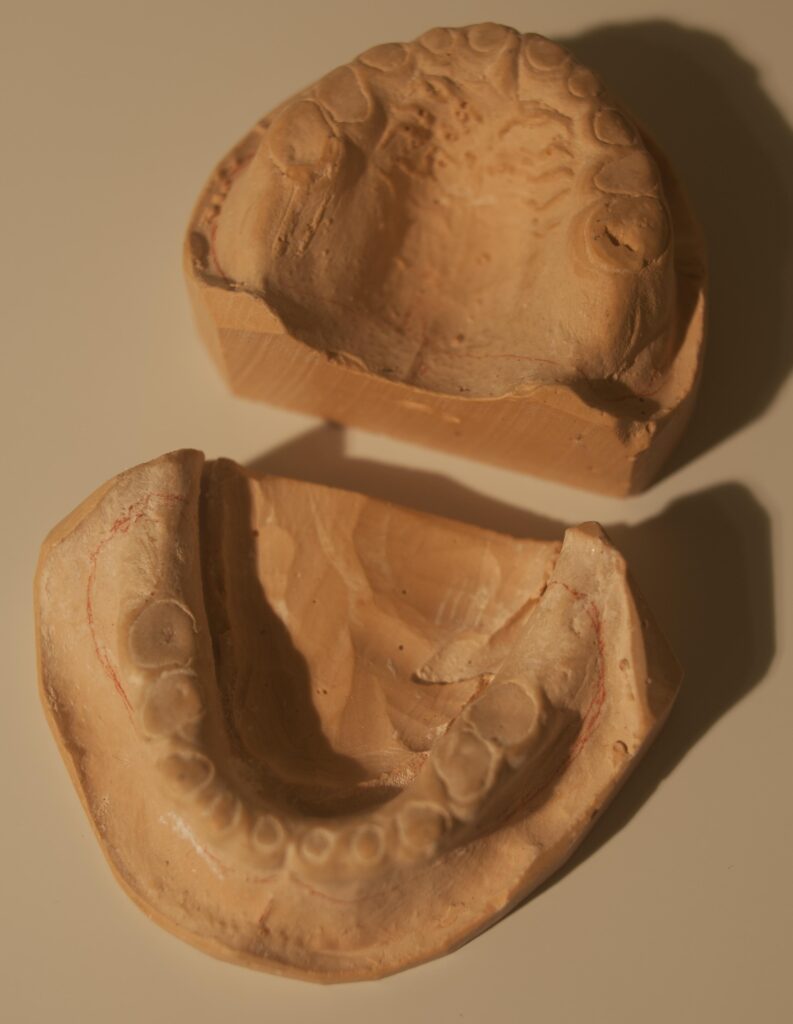
The picture below shows the casts I made originally from the 5-year old boy. It looks like he has NO teeth, but the ovoid circles are the roots of the teeth extending only to the level of the gums.
The X-rays above show that the permanent teeth are coming in, but the primary teeth are just little stumps of roots. Note the absence of a pulp chamber in the first molars.
The challenge with these patients is to try to keep them from destroying the permanent teeth as they erupt, because they will have the same problem and be destroyed by occlusal forces.
For the 5-year old I made a set of complete dentures, to fit OVER the roots, actually an overdenture. You can see the picture of these dentures below. They are so small that most people that see them think they are dentist’s key fobs!

I have these dentures in my possession because after a couple of years, as he grew, I had to make him another set, differently, to accommodate the erupting permanent teeth, to protect them more. So, I kept the old set so I could show my students.
At this point I must say that one of the greatest experiences I have had in my life – and no more justification than this needs exist for my going into dentistry – was when this young boy SMILED for the FIRST TIME. He had NEVER smiled before, as he never had teeth in his mouth long enough before to be seen. Of course, you can smile without teeth, but you know what I mean.
I delivered these dentures to him and he smiled the brightest, most brilliant smile I’ve ever seen! I still get goose bumps thinking about it.
Well – the question remained as to what would happen at school. Kits are, of course, notoriously mean to anyone different. And if a kid doesn’t have any teeth that can be seen, it is a prime situation for harassment. He was bullied horribly, as you can imagine.
So what happened when he went back to school? The other kids actually treated him like he had REALLY GREAT teeth – way better than theirs! But, there was a bonus – he could take his teeth OUT and pass them around. Do you think that would make him seem like a freak? On the contrary, the other kids thought it was a super power! You never know ….
Dentistry for Kids: Bottom Line
This chapter is simply an introduction to some of the issues associated with dentistry for kids. The provision of this to kids is a noble profession.
Kids teeth are really important – and many people assume they are NOT because they will fall out. WHILE they are in the mouth their guidance of the permanent teeth is critical. If they are mistreated and need to be extracted and space is not maintained – it may doom the child to complex orthodontia later that would not otherwise have been necessary.