For more references to the literature on missing teeth, check this Wikipedia page. You may dig into this subject as deeply as you like.
Organization of this Chapter
You May Skip to Whatever Subject Interests You now
Reasons for Missing Teeth
Problems Associated with Missing Teeth
Anterior Teeth
Posterior Teeth
Range of Treatments for Missing Teeth
Anterior Teeth
Posterior Teeth
Bottom Line for Missing Teeth
………………………………………………………………………………………………………………………
Basics
There are many reasons why there might be missing teeth, and there is an equally long list of problems associated with missing teeth. On top of that, there are many ways to replace a tooth – some rather permanent, some removable, and some simply cosmetic. In this chapter we’ll take a look at each of these areas and I hope you will get the idea that a missing tooth should be avoided if at all possible.
Reasons for Missing Teeth
- Lost it in a bar fight. OK – may seem extreme to those of you who aren’t eager to put themselves in harms way – but even in an upscale drinking establishment feathers get ruffled and teeth get lost.
- Sporting accident. I always ask my students why they think that in New England and Canada there are so many teenagers that have partial dentures to replace their upper anterior teeth. Only people from there get the connection. When I was a teenager I used to play ice hockey on frozen lakes every winter. This was not an organized sport, but just neighborhood kids having fun. The problem is that if it were organized we would all be wearing helmets with mouth protection. I still have my upper incisors, but a slap shot to the teeth can cost you – and imagine the pain!
- Deep Decay into the tooth. It may be that the decay is deep enough to require a root canal, and the patient decides not to spend the money and have the tooth extracted instead. Or, the decay may be so deep into the tooth AND pulp chamber that it has decayed external walls of the tooth from the inside, so there is basically zero tooth structure against which to fashion a restoration, even down far to the bone level or below.
- Deep Decay on the root. If there is considerable periodontal recession, so that the roots are exposed, particularly in the furcation, extreme decay in these areas frequently leave the tooth without structure for making reliable margins for any kind of restorative plan. Then loss is inevitable when restoration is not possible.
- Periodontal disease to the point of little attachment. If the gingival attachment and bone have receded far enough down the tooth and root, to the point where there is no bone support for the tooth on the sides or at the apex, and there are few periodontal ligaments left that are keeping the tooth in place, it is time to get it out because it is doomed. I had a patient come in once that had a bridge between a premolar and a second molar, replacing the first molar. The second molar had so much loss of attachment that I could take a piece of dental floss and run it down the back of the tooth, under the apex, and up the front side of the tooth! In other words, there was absolutely NO attachment, and the only thing keeping the tooth in the mouth was the bridge!
- Cracked Tooth. If there is a vertical fracture on the tooth including part of the root, even if we were to do a root canal the leakage of this crack would reinfect the space in the tooth eventually, leading to a recurrence. The detection of a vertical crack is done by having the patient bite down on the suspected part of the tooth, and when they LET UP, then it hurts. This is a clear sign there is a bad fracture.
- Tooth broken off too deep. If the tooth is broken – for example a cusp has broken off, and the gingival limit of the broken area extends below the bone level – that is suggestive of a difficult tooth to restore. It would require a surgical procedure at least to lower the bone level, and if the fracture includes a furcation area, there is a good possibility it is not restorable.
- Tooth Not Needed. Often teeth are extracted for orthodontic reasons, but other teeth are moved into the same place, so no gap is noticed. Or a tooth is not opposing another tooth, maybe a third molar doesn’t have an opposing third molar, and at some point it may be extracted simply because it doesn’t serve any purpose – you can’t chew on it and it doesn’t keep any opposing tooth from erupting more.
- Drug Abuse. Not every drug will cause you to lose teeth – but one, in particular, stands out: methamphetamine – otherwise known as speed and crystal meth. I had my practice in an area that was the meth capital of California – and consequently had many patients with signs of this abuse. While on the faculty of Loma Linda University School of Dentistry I had several students carry out a research project to see just how prevalent the dental consequences of this drug abuse is. We interviewed and photographed over 100 former addicts that were all participating in a rehabilitation center program. Unexpectedly it was evident that if addicts actually took CARE of their mouth, regular brushing, the problems could be minimal. If they just let things go, which seems more likely than it turned out to be, the teeth were destroyed. The PATTERN of decay on the anterior teeth is large brown carious lesions on all teeth near the gumline. The PATTERN of decay on the posterior teeth was decalcification and decay completely around each tooth, until the crown of the tooth just falls off. The drugs seem to anesthetize the tooth, so the loss was not painful or traumatic for the individual. But – the lack of teeth was always a problem in chewing and appearance.
All of these are possible reasons why the patient and dentist will decide not to leave the tooth in place. But there may well be consequences.
Problems Associated with Missing Teeth
For the Anterior Teeth:
Here, of course, the biggest problem is one of esthetics. Just because there is a missing front tooth, the adjacent teeth do not tend to tip into that space – but the missing tooth is obvious enough. On the other hand, if an upper incisor is missing, the lower teeth may rearrange somewhat to fill in that area – this will lead to a crowding situation for the lower teeth, and teeth that look higher than they should be on the lower arch.
Also, certain speech sounds may be compromised by the absence of an upper front tooth – whatever sounds you might try to make that require the tongue to seal the space at the incisal edges, won’t come out quite right. How important this is varies from person to person – there is a contestant right now on a singing competition show that has a missing upper front tooth – and he’s quite good! But, maybe he is avoiding songs with the necessity of making the “F” sound?
For the Posterior Teeth:
One problem with missing back teeth is that during conversation other people may see more of the tooth BEHIND the space than usual.
In this case, if there were to be a filling on the visible side of that molar, as the above illustration shows, it would be more apparent than usual.
For the posterior teeth the most common problems are that the other teeth tend to tip into or erupt into the space created by the missing tooth.
This will not tend to happen as much if there is good fit on the biting surfaces between the remaining teeth. For example, if an upper first molar is missing, the second molar will not tend to move as much into the space IF it has a good cuspal relationship with the lower second molar. This INTERCUSPATION can tend to keep the teeth in the right position for some time.
On the other hand, when a lower molar is missing, while good intercuspation may help, we often find that the second or third molars will tip forward to fill in the space. I don’t actually know why the lower teeth tend to tip more than the upper teeth, however. Studies have shown that lower teeth tend to tip more than upper teeth, but some 20% of individuals don’t show this at all.
The X-ray below illustrates the difficulties attendant upon a missing lower molar.Note that the lower molars, both second and third, have radically tipped into the space!
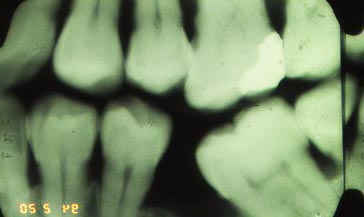
Also, there is a tendency for UNOPPOSED teeth to erupt further into the space created by the missing tooth. For about half of the people with missing teeth, this becomes a significant problem. This is also easy to see happening on the above X-ray.
Supereruption can cause a disharmony in the occlusion, particularly in the excursions of the jaw forward and back and left and right. There will be an interference in the otherwise smooth flow of the arches relative to each other, more frequent “clashing” of teeth and dental trauma, and a reluctance to move the jaw in certain ways that might best fit the facial expression that is being conveyed.
A PRIMARY concern of the effects of missing teeth, is that WHENEVER it is sought to restore the arch, by doing crowns or bridges or implants, the difficulty of the procedure may be compounded when there are teeth that have been allowed to tip.
For example, I had one patient that needed two lower bridges to replace first molars. The second molars were tipped so far toward the empty space that there was no way to fit the bridge to those teeth, they were at completely the wrong angle. In order to make the bridges I had to use orthodontic wires to tip the second molars back up to the direction they were supposed to be. THIS is very difficult to do, because a less than very skilled orthodontics will generally tip the tooth, and they RISE at the same time, so they are hitting “high” when the patient bites down. An orthodontist can actually upright the teeth by making the ROOTS move through the bone, not just move the crown backwards. In the case of my patient, I didn’t have to be that skilled, because I was opening his whole bite anyway, so there was room for the tooth to rise somewhat while tipping back into place. And, I had some professional help from a colleague.
But, typically, a tipped tooth complicates restorations. It can make it more difficult to place an implant to fill the missing space, because there just isn’t enough space to place the implant or make a reasonable sized crown. And if a crown can be made on an implant with the adjacent tooth tipped, there will be such a large space between the tipped tooth and the crown, that the patient will always get food stuck there.
Sometimes, when a first molar is lost very young, the second molar can shift over considerably to fill the missing area. It can function reasonably well if it is not tipped too much and the proximal contact is there, and of reasonable form. The most difficulty for the patient is if the adjacent tooth has shifted ALMOST into adjacent contact. In that case it is likely that food will be pushed through the space between the teeth and pack into the gingival area, causing pain and discomfort for the patient.
For a hypererupted tooth, restoring it with a crown is more complicated as well. So, if a lower first molar is missing and the upper first molar erupts 3 mm beyond ideal to fill the space, making a crown on the upper tooth, perhaps to occlude with a lower bridge or implant that might be done, would probably require reduction of the upper tooth into the pulp chamber! So, the cost of restoring the lower area into reasonable occlusion will be increased by the cost of root canal therapy and a crown on the upper tooth.
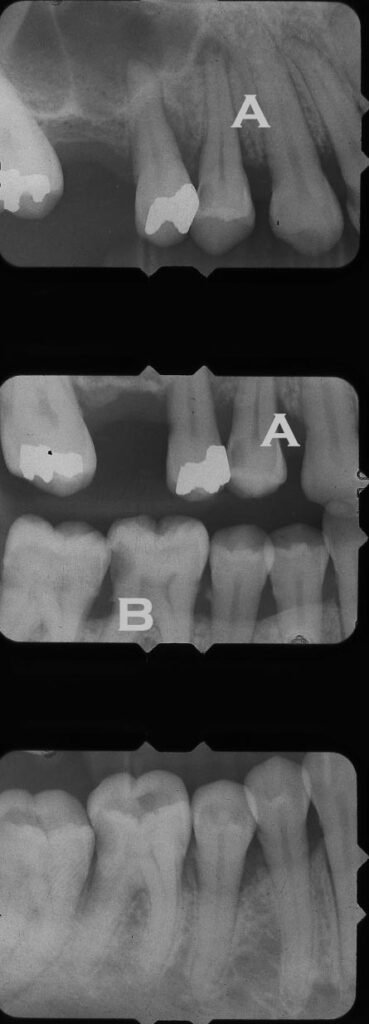
For the case shown in the X-rays above, you might be able to see several issues that have arisen due to the missing first molar on the top.
Range of Treatments for Missing Teeth
For the Anterior Teeth:
Sometimes the problem with the anterior teeth is simply esthetic. There is obviously a missing tooth that need to be replaced. But, it can be done with a cheap appliance, mostly because the functional requirements of that tooth are not great. Unless we are biting into an apple, we don’t do much chewing on the anterior teeth – so something can be done to fill the space without being too expensive or complex.
Visit Chapter V.13 for a detailed discussion and illustrations about all of the options for replacing missing teeth.
The easiest way to replace a missing front tooth, on the upper arch, is a “flipper”. This is an all plastic piece that is worn sort of like an orthodontic retainer – in fact very MUCH like a retainer. It covers part of the palate with a very thin layer of acrylic, it hooks on to at least one tooth on each side using, typically, a little wire with a ball at the end. Onto the plastic palate is connected a replacement plastic tooth, with a little bit of pink plastic where it sits on the gums in the area where the tooth is missing, to look like an extension of the soft tissue up onto the tooth as normal gingiva.
A well made flipper can serve the patient for a long period of time (over a year), but it is really a temporary solution until something more permanent can be afforded. But a flipper can make it so the patient looks pretty much normal, for just a few hundred dollars.
The next level of cost for a replacement would be a metal-framework partial denture. This is similar to the flipper, but the entire thing is far more rigid and strong as it is based on a cast metal substructure. This framework supports clasps onto appropriate teeth that are strong and very retentive – the partial is NOT likely to dislodge under any common circumstances, where a flipper is more uncertain in this regard.
The anterior metal framework partial denture requires a significant amount of labwork, and the cost is significantly higher than for the flipper.
We might also do a bridge to connect the replacement for the missing tooth to the adjacent teeth. This is a permanent and fixed restoration, it does not have to be removed at night like a partial denture or flipper.
One type of anterior bridge is a “Maryland Bridge” – where the adjacent teeth do not have to be reduced much, because the bridge is secured to those teeth by adhesive techniques. This is also referred to as a Resin Bonded Bridge. There is usually a metal framework that is bonded to the adjacent teeth, and supports the replacement tooth, or pontic, which can be made of plastic or porcelain. The esthetics can be quite good – the laboratory technician can even make the replacement tooth himself out of porcelain, so it is a customized match to the other teeth in the arch.
When a resin-bonded bridge is done with a metal framework on teeth that are mobile because of periodontal disease, there can be a problem. If the adjacent teeth are mobile, the rigid framework of the bridge will cause stresses to build up at the cemented junction between the framework and the adjacent teeth, to which it is cemented. I have found this to be the case with lower incisors especially. One of my patients had a traditional metal framework Maryland Bridge that kept falling off and she came to me to see if I could take care of the problem. I elected to use a COMPOSITE FRAMEWORK, which was more flexible, and the success was dramatically improved. While she had been having the metal framework bridges fall off in weeks each time, I am not aware that the flexible framework bridge ever did fall off, certainly not in the two years that I was able to track that patient.
Of course, the traditional bridge for the anterior teeth might be appropriate as well. In this case, maybe the adjacent teeth are compromised and could use crowns anyway – but in any instance, both adjacent teeth are prepared for traditional crown restorations (as we’ll see how in Chapter V.7), and a restoration is made with porcelain over a metal framework for all three teeth. This is almost three times the cost of a Maryland Bridge, and is much more destructive and aggressive – but may be appropriate.
The final way to restore a missing anterior tooth is to place an implant in the bone and then restore it with a single crown of porcelain. Sometimes it is even possible to extract a tooth, place an implant and do a CAD/CAM crown (visit Chapter VII.4 for a discussion of high technology in dentistry) all in one visit to the dentist! If the crown would be placed under too much load during function after installation, this is not a good idea, but there are times where it works out fine.
Typically, once the implant is placed, it is allowed to integrate with the bone of the arch for a few months before a crown is made, and during that time something like a flipper can be used over the implant area so the patient will look normal during healing.
Posterior Tooth Replacement:
For a missing posterior tooth we have many of the same choices as for an anterior tooth, but the flipper is not a viable choice. The main problem is that the posterior teeth are in FUNCTION – they have work to do, chewing particularly. Whatever holds the replacement tooth in place needs to be far more robust than for a simple flipper for the upper front teeth.
The standard choices for missing posterior teeth are removable partial denture, bridge and implant with crown.
The Maryland, or Resin-Bonded Bridge, can sometimes be used with first premolars, but is not recommended for more posteriorly placed teeth due to the increased functional load.
In appropriate sections of this site we will look at specific methods for partial dentures, for bridges and for implant-supported crowns. But, as I’ve already alluded to, whenever the open area caused by loss of a tooth is allowed to stay unfilled for a long time, the simplicity and even practicality of replacing it using any of these methods is called into question.
Bottom Line
If you loose a tooth for whatever reason, take care of the SPACE. Retain that space somehow so that the surrounding teeth do not shift, causing complications in whatever restoration you may eventually get. When kids lose primary teeth, we need to place some kind of space-maintaining device so that the permanent teeth will erupt in the correct place under the remaining primary teeth. Visit Chapter V.19 for more on this. For adults the need for space-maintenance is equally important for most people, if not for everyone.
For more on Tooth Replacement, visit Chapter V.13. For more on Orthodontics, visit Chapter V.17.