If you want to explore the TMJ (Temporomandibular Joint) in more detail I would recommend the Wikipedia article on the TMJ. It includes many links and references that are responsibly sourced.
Organization of this Chapter
Basics
The Condyle
The Socket (Glenoid Fossa)
The Disc
The Hinge-Slide Motion
Bottom Line for the TMJ
………………………………………………………………………………………………………………………..
The Basics
If you felt the condyle of the TMJ with your finger in the last Chapter, you may have noticed that with small openings the condyle stays in place, merely rotating. But with larger opening you can feel it slide downward. Note also that there is a fibrous disc between the condyle and the socket or fossa which moves with the condyle. Disorders of the condyle often involve this disc, and the clicking and popping that many people experience upon opening and closing the mouth has to do with this disc slipping in and out of its desired position.
In order for us to find out more about this joint, we will look at each of the main components individually.
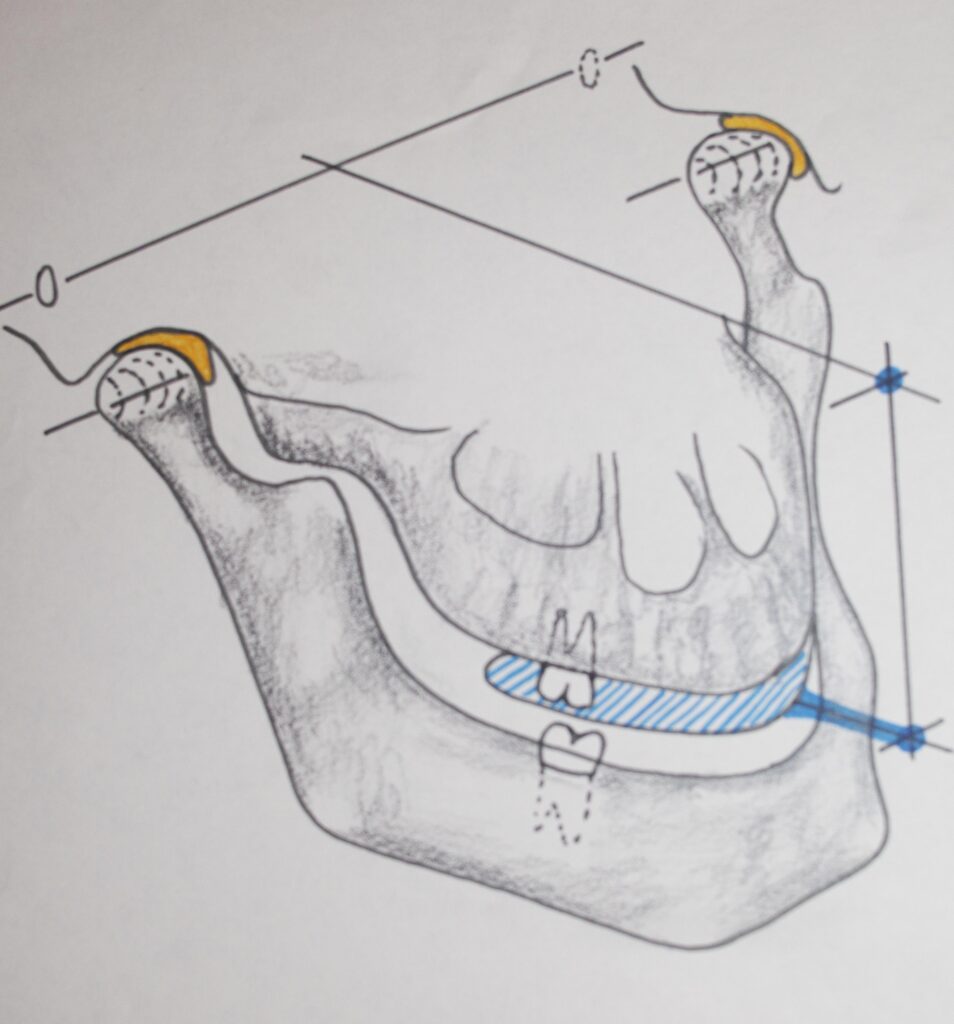
In the diagram above you can also see illustrated the ear-holes behind the TMJ about 10 mm. Also, it is demonstrated that when we work with the teeth sometimes we need to know exactly where they ARE relative to the TMJ, where the jaws hinge. We use a device, called an articulator, to relate the teeth to the TMJ so we can simulate the movement of the jaws, and hence can mimic the movement of the upper and lower teeth relative to each other.

The picture below shows an actual articulator that is holding casts for the fabrication of a full denture.

The TMJ: The Condyle
The picture below shows more detail than was possible in the sketch of the mandible that we looked at previously. What you see is the ideal, rounded shape that conforms best with the disc surface, and rotates most smoothly.
The condyle doesn’t always look like this. When the disc becomes damaged for some reason (perhaps an auto accident or a traumatic bite) then the condyle often will take on an irregular appearance due to erosion of part of its surface by bone-eating cells. These cells are always at work, but are normally counterbalanced by bone-forming cells. But in situations where damage has occurred this balance can be disturbed. Many times the condyle must be replaced by artificial materials (Teflon for example) in a surgical procedure.

One interesting lesson that can be learned from the paragraph above is that bone is not just an inert scaffolding upon which our bodies are hung, it is a dynamically formed and resorbed substance. In the case of infections, like in the gum pockets, the bone that is nearby will retreat. In case of mechanical damage the bone will resorb. When something pulls on bone, on the other hand, it will grow in the direction of the pull. That’s what forms the coronoid process.
The TMJ: The Socket (Glenoid Fossa)
The socket for the TMJ is immediately in front of the ear, again, feel the movement of the condyle in the socket with your finger. The picture above shows the general shape of the socket. The basic shape of the socket has two parts, the hinging part which is the rounded part toward the top, and the sliding part which is the sloping part toward the nose or front. It is of interest that the sloping part will have a different angle from person to person. Sometimes the dentist actually has to measure this angle to see how the teeth will move with condyle movement. It is vital to know then when replacing many of the natural teeth with artificial teeth.
In the picture below you can see how the condyle and disc have slid down this slope, leaving the top part of the socket open. This is a simplistic but good visual picture of the TMJ movement, and a good illustration of its complexity.

The TMJ: The Disc
Now that we’ve seen the condyle and the socket, we need to study the disc that fits between them. Its general shape is kind of like a funny-shaped donut, with the condyle fitting in the thinner central section. When the jaw hinges up and down the condyle merely rotates in the disc, but when opening wide or shifting the chin from side to side, the condyle AND THE DISC will slide down the slope of the Fossa, as seen in the picture above.
The disc is controlled to some extent by muscles that are attached to it in the front, and it is also connected loosely to the bone toward the back. Part of the same muscle that is used to pull the condyle forward and down the slope also serves to move the disc forward. When the disc does NOT move with the condyle, it is a disorder that can result in discomfort in the joint, and often something needs to be done to correct that.
The TMJ: The Hinge-Slide Motion
The pictures of the human skull below show two positions of the joint, one corresponding to swallowing, or closed mouth, the other corresponding to wide open. Note that I have made “discs” out of a rubber material so that things fit together better. The path of movement of the jaw is toward the left. Note that this represents what is happening to ONE of the joints – and this will be the same for both ONLY if there is no side-to-side deviation of the chin. A pure lateral movement of the chin will cause the joint toward which the chin is moving to remain in the closed position, merely rotating about a vertical axis, while the opposite joint (shown) will rotate about a horizontal axis while sliding down the slope and arcing in the direction of chin movement. The second picture shows the mandible moving laterally in more detail. A pure forward shift of the chin causes both joints to slide down the slope without rotation about the horizontal axis.


Another important consideration is what the teeth are doing while the mouth is opened, closed, or shifted laterally or forward. The picture of the skull above gives an idea of the plane of the teeth in relationship to the joints. The SLOPE of the fossa toward the front, where the condyle slides in pure forward movement or when moving toward the opposite side, in this case, determines the precise movement of the teeth, upper relative to lower. In cases where most of the teeth are replaced artificially, the dentist often will need to be aware of the specific joint anatomical situation for the individual patient so that the tooth-to-tooth relationship can be maintained appropriately during important jaw movements.
The next Chapter will deal with important concepts about the relationship between the teeth in the two dental arches. Many times the bite relationships are the most misunderstood by students of dentistry and by practicing dentists as well. There is also considerable controversy in the field about the importance of bite relationships.
Bottom Line for The TMJ
Without a smoothly operating joint, we would be hard pressed as humans to function in society, or even live. Eating requires a very precise positioning of the joint during every bite and chew. Smiling requires a very precise position of the joint for just the right tooth opening to express our emotions. Speaking requires a very precise positioning of the joint to allow the formation and enunciation of words for basic communication.
Anything that disrupts the ability of the joint to position itself well, is potentially disastrous for us. In Chapter III.6 we’ll discuss disorders of the joint and the pains that may be associated.