The core dental buildup replaces missing tooth structure so that a crown can be made over that, with enough retention. Many dentists have made the habit of just filling in a little bit of missing structure and billing the patient or insurance for a buildup as well as the crown. But there are times where virtually the entire visible part of the tooth must be rebuilt before any crown can be attempted.
In the former case, charging the patient is not reasonable, but in the latter case it is wholly justified. Insurance companies can’t necessarily tell the difference, so they often don’t pay for work that really needs to be done, that might take up to an additional half hour of the dentist’s time.
Note that it is often possible to USE the missing parts of the tooth as retentive features for an ONLAY, rather than filling them in and doing a full crown over everything. But many dentists have less experience with onlay restorations and do the much more aggressive full crown procedure.
Organization of this Chapter
You May Skip to Whatever Subject Interests You Now
Basics
Retentive Pins and the Ill-conceived Alternative
Composite Resin Buildups
Buildup for Partially Broken Down Teeth
For root-canal Treated Teeth
For Vital Teeth
Bottom Line for Dental Buildups
………………………………………………………………………………………………………………………
The Dental Buildup: Basics
When a tooth needs a crown but is too badly broken down for there to be enough tooth structure left to support a crown, missing tooth structure must be rebuilt before it can be prepared for a crown. This rebuilding of the tooth is termed a “buildup”.
When a buildup is done, it needs to be secured to the tooth well, because often it is the buildup that is securing the crown to the tooth. When the buildup dislodges, the crown comes off along with it.
I had a patient come in once with a crown in her hand, and inside the crown was almost filled with amalgam. Well – the dentist who made the crown had done an amalgam buildup and then made the crown to fit over it, but the buildup had been inadequately secured to the tooth!
When I looked in the patient’s mouth I saw practically nothing of the tooth. There was just a short wall, no more than 1 mm tall anywhere, ringing the entire tooth. There were no cusps at all – everything was just a flat surface 1 mm above the level of the gingiva. Now – you might be thinking about where the rest of the tooth went and where the pulp chamber was. You would be correct to question that – the fact is I have no idea what happened to the rest of the tooth. Sometimes parts of teeth erode away after lots of breakage and chipping, and after the tooth is ignored for long enough, what is left is pretty well flattened and smoothed out.
I once had a patient that had both first and second premolars on one side of the upper arch gone except just a small bit of root showing above the gumline in each case. The root substance was smooth and polished and decay free. How they got that way is also a mystery.
The question of the pulp chamber is also curious – but you have more means to figure this after earlier discussions (visit Chapters II.2 and III.3, for discussion of the normal pulp and infected pulp, respectively). As the tooth is assaulted by decay and maybe even trauma, the pulp moves, by virtue of the odontoblasts within forming more dentin. The pulp recedes faster than the invasion, it is hoped.
The Dental Buildup: Retentive Pins and the Ill-conceived Alternative
In the case of the patient with the crown that had fallen off, it was abundantly clear that the dentist who had done the buildup had done it poorly – after all, it fell off. How SHOULD it have been done? Well – some way needed to be found to retain the buildup to what is left of the tooth. The buildup being amalgam, the dentist could have placed small screwed pins in each of the corners of the tooth, in dentin, and then build up the amalgam over the pins. This is a technique that has stood the test of time for many decades. The dentist drills small holes into the dentin and then screws the pin into the hole, gently, so as to not cause any stress on the tooth by overtightening. This is more graphically discussed in Chapter V.2)
The pins I generally used were no more than .5 mm in diameter and a few mm long. After placing them gently by hand, they are bent slightly toward the center of the tooth, so that when the buildup is done, they are completely embedded in the amalgam. It must also be considered that a crown preparation will be done OVER the amalgam buildup, removing a mm or so of it on each of the four axial, side, walls. When the crown preparation is done, it would be best if the dentist didn’t cut off the pins!
Retentive pins have serve dentists and their patients for generations, but in the late 80s, with the advent of adhesive dentistry, dental manufacturers and even dental school faculty formed the opinion that we could do without pins if we adhesively bonded the amalgam buildup to the tooth. This technique was given the name amalgam bonding, and a material was even commercially offered called Amalgambond. I suspect this is what the previous dentist had done for my crown fell off patient. Visit Chapter V.4 for a discussion of adhesive dentistry.

When I looked at the remaining tooth structure for this patient, I was specifically looking for any signs that pins had been placed and been cut off or broken off – and saw nothing. So the most likely thing is that the dentist tried amalgam bonding. The research in this area has not demonstrated enough convincing successes to take such a chance in a case like this, where there is virtually NO mechanical retention for the amalgam onto the remaining tooth. And, certainly, this case seems to suggest finding another way to proceed.
It is likely that in the cases where amalgam bonding is attempted, the connection between the bonding cement and the amalgam is the weak link. It was thought that the composite resin material would make fins up into the bulk of the amalgam as it is condensed, and this would provide a mechanical link, but this is probably not as effective as we once thought it would be.
More details of the situation for this patient may be found in Chapter V.4. But the bottom line for this Chapter is that a buildup for a crown must be done so that it is WELL retained on the tooth, and anything less will compromise the crown, and potentially cost the patient a lot of money.
Composite Resin Dental Buildups
One must think seriously about using the composite resin or plastic materials for a buildup instead of amalgam. The amalgam is a much more rigid material, and I would say that when a large part of the retention of the crown is provided by the buildup material, amalgam is superior. But dentists will often use composite materials that are designed to be used for buildups, at least when there is still enough tooth structure left to “share the load”.
Dentists have choices to make, and various approaches and materials that can be used to solve particular problems in individual patients, but no one material or method works for every circumstance!
Dental Buildups for Partially Broken Down Teeth
When a tooth is partially broken down, it has enough tooth structure left to at least partially support a crown. How a buildup is done to complete the task of fully supporting the crown is an individual problem.
Buildup when the tooth has had a “root canal”
Here we have access to the pulp chamber and root canals of the tooth for retention of a buildup. No matter how much or little of the tooth is left above the gumline, the internal portion of the tooth provides great retention for a buildup, and hence great retention for the crown.
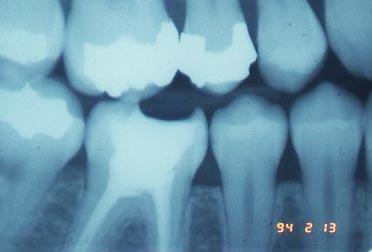
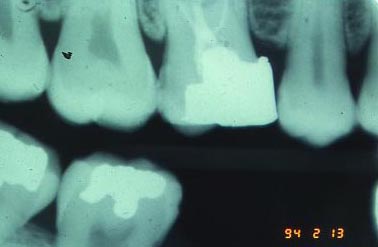
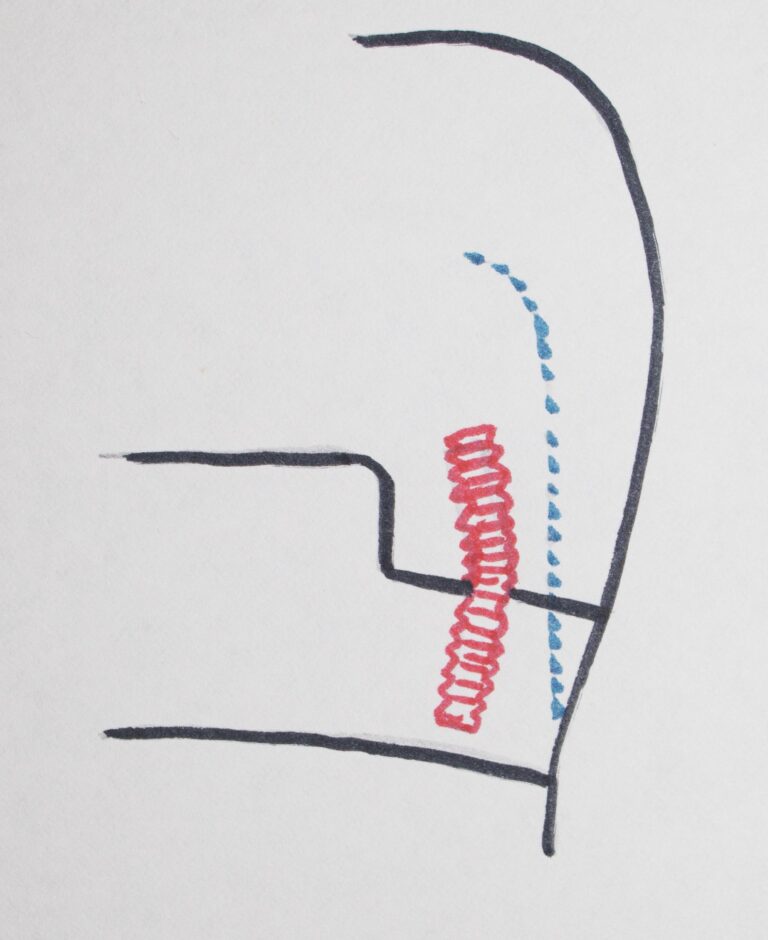
Depending on the form of the pulp chamber volume, we may be able to just fill the chamber with some buildup material, either amalgam or a composite material, and bring the height up close to the opposing tooth, maximizing the height of the walls that can be made to support the crown. On the other hand, for a non-vital tooth (where the RCT has been done), we might not have all of the walls of the pulp chamber intact (see second X-ray above), and then it is common practice to place a POST in the largest of the canals and then the post will be a retentive feature for the buildup. It’s kind of like a huge pin, that we discussed earlier.
For the lower molars, the canal toward the back of the mouth is largest and often used to place a post. For the upper molars, the canal toward the palate is the largest and straightest and is often used. There are different systems that can be used for this. One type of post uses a screwed-in post, where the canal is drilled out first and the post screwed in. A second type of post is the CEMENTED POST – where the canal is drilled to fit a prefabricated post which is then cemented into this hole. A third way to create a post is used mostly for anterior teeth where the canals are very tapered toward the apex – in this case neither of these first systems may work well, and we need to fabricate a post in the lab that is custom designed for the root canal. This cast-post is then cemented in, and the crown is prepared over it.

My personal preference is toward cemented posts for the posteriors and cast-posts when needed for the anteriors, but I make the post and the crown at the same time. This is generally not done and requires a particularly good laboratory technician and careful preparation, but serves the patient well.
For the screw post I got a good lesson from the dentist I associated with right out of dental school. He used to simply screw the post lightly into the canal and then condense the buildup material over it, typically a composite material that sets on its own rather than needing light. I have no problem with the buildup material, however he used to place the post in ALL cases, just because he could charge the patient or insurance company extra for that! I once saw an X-ray of a crown done with a screw-post retained buildup, where the screw was clearly not even IN the tooth, it was just floating around in the buildup, contributing nothing to the retention at all!
Dental Buildups when the tooth has NOT had a “root canal” – it is still vital:
Now we have a situation where there isn’t enough remaining strong tooth structure to support a crown, but we can supplement it with some buildup material, either composite or amalgam. If using composite, it would be wise to not rely totally on adhesive bonding, so mechanical retentive features are generally used, whereas for amalgam we will rely totally on mechanical retention.
Mechanical retention for a buildup may consist of boxes or slots or grooves or pins or parts of remaining cusps that work like pins – we use everything we can find that will secure the buildup material soundly to the tooth. If the tooth originally had a class II restoration so it has box forms on both sides near the adjacent teeth, we will make sure these boxes converge toward the occlusal so nothing condensed in can come out. If we are missing a cusp in a corner of the tooth, we may flatten out an area where we can put a pin, making sure that the buildup is formed totally around the pin so it has its greatest effect. If there is a cusp missing we will often place an additional undercut box form between it and an adjacent, more complete, cusp.
See Chapter V.2 for some illustrations of retentive features that may be used to secure amalgam into a tooth to replace one of more cusps. These techniques are very similar to what we do for a buildup. With a BIG caveat – as the next paragraph presents.
Above all, and obviously, we must make sure that when the tooth is prepared for the crown, we don’t cut away the retentive features we placed for the buildup! The retentive features that we use to restore cusps with amalgam need to be done so they are STILL retentive when the tooth has been reduced on the outside surfaces for the crown!
A little planning and engineering and seeing things a little ahead is all it takes to do this in a way that will be quite effective.
Bottom Line for Dental Buildups
Building a tooth up is necessary if there is not enough tooth structure left to support the crown on its own.
The materials used for dental buildups can be either amalgam or composite – the choice depending on the precise circumstances. Most dentists these days will tend toward composite because of its ease and speed.
For a non-vital, root-canal treated tooth, the buildup material may be placed directly into the empty pulp chamber, or a post may be placed first into one canal and then the buildup is done over this post for more retention. The choice will largely depend on how many side walls of the tooth are missing.
For vital teeth, where the pulp chamber is still intact, we need to do a buildup as if we were restoring the tooth to full contour without planning a crown. In certain cases a composite material would do well, but when there is VERY little tooth structure remaining and the buildup will be LARGELY responsible for the retention of the crown, best to use amalgam.
The design of the preparation FOR the buildup of a vital tooth requires some mechanical thinking on the part of the dentist. The forces that will be exerted on the crown need to be considered in terms of how those forces are transmitted to the buildup, and to the features that retain that buildup.