Periodontal therapy at home means removing plaque – the sticky layer of bacteria-loaded surrounding the teeth – on a daily basis. When plaque remains too long, hard deposits are made which limit your ability to keep your tooth surfaces clean enough to avoid periodontal disease. The dentist of hygienist are responsible for removing the hard calculus deposits from your teeth – but if they do not on a regular basis, a change in your appearance will result, either through gum recession or tooth loss.
An excellent paper on periodontal therapy has been published with many references to the primary literature. For those that want to explore this topic more deeply, I recommend you look at this.
Organization of this Chapter
You May Skip to Whatever Subject Interests You Now
Basics
Plaque Removal
Home Care
Flossing
Flossing Technique
Electric Toothbrushes
Brushing Technique
Complicating Factors
Toothpastes
Professional Plaque Removal?
Calculus or Tartar
Removal of Calculus
The Cleaning Appointment
Root Planing
More Serious Situations
Bottom Line for Periodontic Therapy
……………………………………………………………………………………………………………………….
Periodontal Therapy: Basics
It hasn’t been mentioned before, but the term “periodontal” comes from things being NEAR the tooth, or around it. Like perinatal things that happen near birth.
We’ve discussed the design of the periodontal ligaments and how they are instrumental in the support of the tooth in the bone, and how important the level of the bone is. Visit Chapter II.3 for a discussion of normal structures.
Also, we’ve seen the nature of the information we need to collect about each tooth in the mouth so we can have an idea how serious the periodontal condition is. If the periodontium is infected badly with harmful bacteria and they are not cleared away – whatever damage they cause is essentially permanent! Visit Chapter IV.4 for a discussion of periodontal charting.
As harmful bacteria congregate around the tooth, they do several things that are bad. One; those bacteria that produce acid will tend to demineralize the enamel of the tooth, and then the bacteria can enter the area and continue their deprivations unabashed – leading to extensive decay. Two; those bacteria which prefer to live away from exposure to oxygen in the air, can set up housekeeping in the periodontal pocket – where they release chemicals that harm the gingiva, the gingival attachment to the tooth, and even the bone which holds the tooth. For a discussion of the disease states that affect the periodontal support of the teeth, visit Chapter III.2.
In this chapter we will be concerned with what can be done to those subgingival, anaerobic bacteria that are of special concern to the periodontal tissues, and how to arrest the damage done!
Periodontal Therapy: Plaque Removal
As bacteria are allowed to congregate around a tooth, there is a sticky, gooey substance that forms, consisting of bacteria cells and various polysaccharides, called Plaque. It is EASILY removed, one just needs the will to do this.
Plaque will coat the teeth, on the facial and lingual surfaces, as well as those surfaces between adjacent teeth.
Home Care
Brushing the teeth is effective at removing the plaque and associated bacteria from the facial and lingual surfaces, but removing it from the areas between the teeth is more difficult. The space between adjacent teeth, below, or gingival to the contact area, and above the gumline, is a potentially open area where plaque can enjoy some safety.
When you are young, this space below the contact, called the gingival embrasure, can only be accessed by dental floss, because it is a small area – as it were bounded by the two teeth, the contact and the gingiva, which tends to be high in young people. But for older people, it can be accessed by little brushes, for example the Proxibrush. It is like a toothbrush with just one big bristle – like a miniature baby bottle brush. They come in various sizes, and can be pushed between the teeth to brush out all plaque.
Flossing
Dental floss is your first line of defense against plaque buildup. The object of using floss is NOT to go through the contact and back again. Even the dental hygienist may not seem to note the subtle difference between simply going through the contact, and what you DO when the floss is below the contact area. The purpose of the floss (as the hygienist should teach you) is to SCRAPE the sides of the teeth that are touching – each of them in turn. The floss is pushed through the contact and then pulled tightly against each adjacent tooth surface in turn, where it is run up and down – up toward the contact and downward into the gingiva as far as comfortable. In this way the floss will remove all of the plaque on each tooth.
What KINDS of floss should you use? There are three main categories: waxed floss, unwaxed floss, and teflon-coated floss. I would stick to the first. The waxing of the floss is what helps it slide through the contact without shredding, and yet the wax does not interfere with the effective removal of plaque. The unwaxed floss tends to shred more and I never found it appealing. The teflon-coated floss is great at going through the contact, but when the plaque is rather “stiff” or presents a more solid mass than the softer variety, I’ve actually seen this type of floss simply glide OVER the plaque, in a patient’s mouth!
The use of dental floss DOES require some manual dexterity – there is no denying that. I’ve had third molars most of my life, and to get the floss between those and second molars requires some serious reaching.
Floss Technique
The basic procedure, which the dental hygienist should help you learn, is to get a LOT of floss, and wrap it around the palms of both hands, extending the loose length so it is supported by the TIPS of your left and right fingers, either index or middle fingers, or both. With the floss being held tight because it is wrapped around the palms, the fingers only have to DIRECT and place the floss in the right area.
Toothbrushing, naturally, is important as well. There is nothing as effective in eliminating plaque from the OCCLUSAL surfaces of the posterior teeth, and it will readily remove plaque from the facial and lingual surfaces but the only thing that will work in the contact areas is floss.
Electric Toothbrushes
The TECHNIQUE of toothbrushing is not as important these days, because electric toothbrushes are so readily available. I used to provide one in my dental practice where each of the tufts rotated independently – it was a really cool design and very effective. That particular device was not as well engineered as could be, so it disappeared eventually from the market.
Electric Toothbrushes these days come in two different versions – the rotation kind and the oscillating kind. Both are available as cordless models with a small charging stand. My preference is for the oscillating, up and down kind, which sweeps across the tooth vertically and is potentially more effective at getting into the embrasures. But I am sure that either style will be effective in plaque elimination.
Brushing Technique
For those still using hand toothbrushes, an up and down motion is OK, but a small circulating motion is most effective. And, don’t miss the chance to massage the gums at the same time.
When I was in dental school we had in instructor in the hygiene department that brushed all of the dental student’s teeth, one time. It was a glorious experience! While at first it may seem like you are being treated like a kid, how can you teach others to do something when you haven’t experienced the teaching process yourself? I always brushed my patient’s teeth as a demonstration of what it FEELS like. And – this person that taught us by example, used to make a living brushing the teeth of Secret Service agents! I don’t really know how she got from there to doing the same in dental school.
All of the above is called HOME CARE. This is what WE do at home to take care of our teeth. At least we are supposed to. It is SO easy to blow it off for a day or two, but there is always a price to pay.
Complicating Factors
Certain conditions in the mouth make adequate home care more challenging. Perhaps you have braces with brackets and archwires. Perhaps you have implant-supported crowns or bridges. Perhaps you have bridges supported by natural teeth, and the underneath part cannot be reached through the contact because there is no contact. Or maybe you have so much recession that there is lots of space between the teeth under the contact area, or furcations are exposed.
The dentist will want to know that you have a firm grasp on the importance of home care, at a level commensurate with the dental conditions in your mouth, and the procedures and appliances that may be involved in your dental treatment. If you cannot take care of your teeth at home, you will not be able to take care of an implant – and the consequences could be the loss of a $5000 investment!
The dentist or dental hygienist can look at your teeth when you come in and see if you are doing a fair job of plaque removal. Even if you brush your teeth just before coming to the dentist (after not for two days), there will be signs that you are being negligent. The hygienist can take a PLAQUE SCORE using a red die that colors the plaque specifically – but they can also just look at the condition of your gingiva.
If your gingiva are red, bleeding and swollen, you have not been taking good care of your teeth.
Toothpastes
I will not attempt to scientifically rationalize all of the different types of toothpastes that are currently on the market, or evaluate every marketing claim with scholarly research.
Some toothpastes are designed to help with decay prevention by hardening the enamel – utilizing fluoride in various concentrations. Over the counter products are allowed a maximum percentage of fluoride, and those that approach this percentage are rightly sold as more decay preventive, or used for “enamel hardening”.
Some toothpastes are designed with ingredients that will tend to reduce the concentration of gum disease causing bacteria in the mouth – and these would be for people with periodontal problems.
Some toothpastes are designed to help with root SENSITIVITY – the most well known example of this is Sensodyne.
And, there are always the WHITENING toothpastes. The first of these was called Rembrandt and it was sold by a small company in California that I knew pretty well. They had many other products, but THIS product is what made their fortune. They sold it for something like $8 per tube back in the 90s, and people bought it like hotcakes. Did it actually whiten the teeth? Maybe not so most people would notice – but even if it did not, it made people FEEL more attractive.
More on the subject of toothpastes will be coming to the site soon.
Professional Plaque Removal?
There is not much that the hygienist in the dental office can do that you can’t do at home, as far as plaque removal is concerned. She may floss your teeth and use a polishing cup to polish all accessible surfaces, making the adherence less likely for a few days – but mostly it is up to YOU.
What the hygienist DOES do that you cannot do at home, is removal of the HARD deposits that are made within the plaque if allowed to sit in place too long.
Periodontal Therapy: Removal of Calculus or Tartar – the Hard Deposits YOU Cannot Remove
As mentioned above – when the plaque is allowed to sit in place for too long a period of time, the bacteria start to create mineralized structures adhering tightly to the enamel or cementum surfaces of the crown of the tooth or the root, whatever is accessible.
Think of the sea creatures that make shells and barnacles. These are simple creatures that have a great skill in creating mineralized structures. The amazing variety of shells types speaks volumes about how diversified and evolved these creatures are. The barnacles on pilings under sea water are just less interesting versions of the same things – the little conical constructions that cover such underwater surfaces are very much like calculus on a tooth. The creatures that make barnacle shells are just making their HOME! The creatures that inhabit our mouth are doing precisely the same thing – they make a mineralized edifice that is firmly attached to the tooth so that WE cannot remove it ourselves.
So, this calculus deposit, once allowed to form, remains in place until the next visit to the dentist. The bacteria that inhabit the calculus are then in place for a potentially long period of time, making chemical irritants that damage the gingiva and attachment to the teeth.
The Removal of Calculus
Cleaning – the Prophylaxis Appointment
For this removal, the nature of the procedure depends on where it is located. If the calculus is on the enamel, it is generally above the gingival level and can be removed without impinging on this sensitive soft tissue. In fact, when there is calculus present near the tissue, you can count on the tissue being inflamed – for there are bacteria constantly right there as foreign bodies that the body will attempt to fight.
If the calculus is above or at the gingiva it can be removed painlessly by using scalers. A scaler is a little hooked scraping device with a sharp point and sharp edges that can be pulled up along the enamel surface and the calculus will normally readily pop off. Sometimes the calculus is on the enamel but somewhat below the gingiva – and if this is the case, careful removal of it usually means there is little discomfort to the patient, and no need for anesthesia.
When calculus is removed above the gingiva, or somewhat below the gingival level, it is part of a DENTAL CLEANING, or PROPHYLAXIS. The hygienist or dentist will remove the calculus on the facial and lingual surfaces of every tooth, and in the areas between the teeth, and on the occlusal surfaces, and then polish the teeth and you are done.
Root Planing – Removal of Subgingival Calculus
As distinguished from the standard cleaning, if the calculus is distinctly below the gingival level, significantly down in the periodontal pocket, and found on the root surface itself – the removal of that would be termed ROOT PLANING. This uses specially designed instruments that scrape like scalers, but have a rounded tip so as not to damage the gingiva. These CURETTES have different shapes to enable them to reach into all different areas of the mouth. A hygienist or dentist will often use five or six different curettes in order to reach every place on every tooth.
Since the professional is working considerably below the gumline, and maybe as much as 8 mm below it if the pocket is deep enough and the calculus is close to the bottom of the pocket, there is cause for PAIN from two sources. First, pain may well ensue because these soft tissues are really inflamed, and inflamed tissue hurts (splinter in finger). Second, when the professional scrapes the calculus off of the ROOT SURFACE, the cementum is removed as well, and the dentin is very sensitive, as the tubules with the nerves in side are exposed. Root Planing requires anesthesia.
Part of the root planing procedure is to SMOOTH the root surface so that calculus will have a harder time adhering to it next time. There WILL be a next time, unless the patient keeps the site clean in every way they can.
Root Planing is generally done one quadrant at a time, because it takes a long time to clean every surface in each quadrant, and because we don’t want to anesthetize too many quadrants at one appointment.
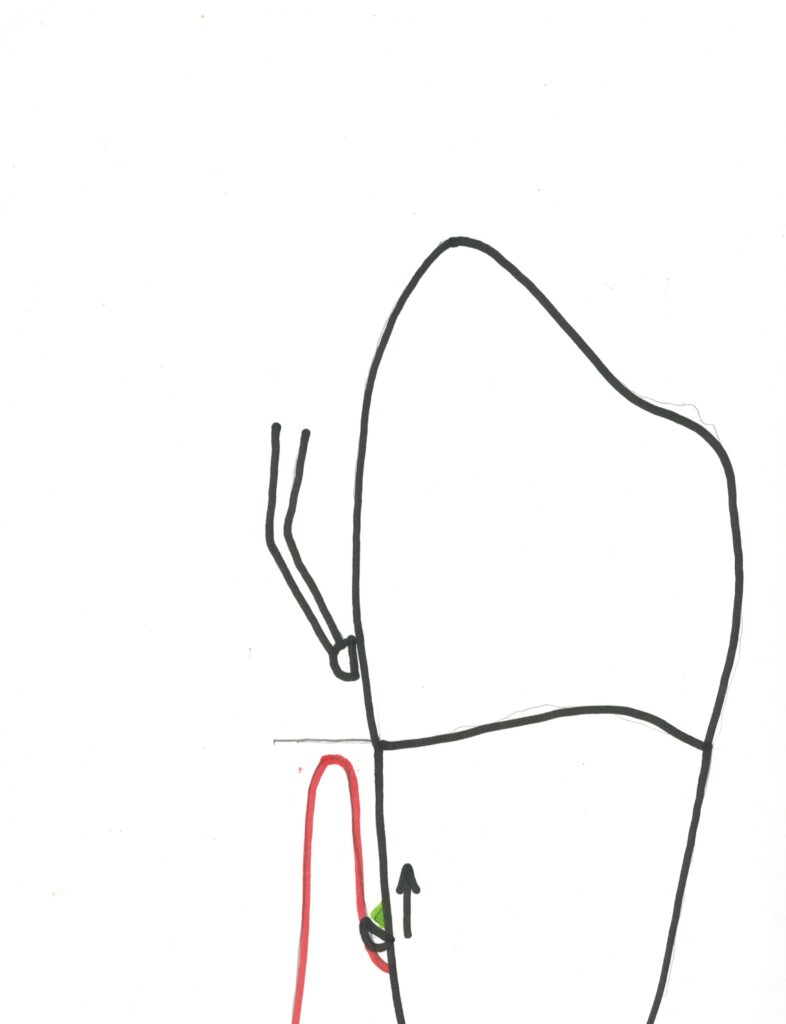
The basic technique is illustrated in the diagram below. The curette is adapted to the surface the tooth, moved subgingivally until the dentist or hygienist can feel it slide BELOW the level of the calculus, and then the instrument is tipped so the edge is against the tooth as it is PULLED UPWARD. This scraping action is what removes the calculus, although it may take several attempts. An explorer is used to determine how smooth the toot is after treatment, and that the calculus has been completely removed all around the tooth.
I will mention here also another term that is in, unfortunately, wide use: DEEP CLEANING. A normal prophylaxis appointment, dental cleaning, should go far toward taking care of the needs of the teeth, unless root planing is required. I don’t believe in charging more for a more “significant” cleaning visit, when anything that can be done to the whole mouth in one visit is a standard dental cleaning appointment.
On the other hand, if you have to do the calculus removal quadrant by quadrant because the calculus is ON THE ROOT, that is root planing.
In my opinion, there is nothing between these two.
More Serious Cases the Hygienist Cannot Manage
Normally it is figured that the hygienist or dentist can remove calculus at the bottom of a pocket 5 or 6 mm below the height of the gingiva. That involves reaching down pretty far into a deep pocket, feeling the piece of calculus, and bringing the instrument back out, scraping off the calculus on the way. There is a lot of skill to this procedure – and not everyone is equally gifted in this technique.
But, if you have calculus near the bottom of a 6-8 mm pocket, the hygienist will TRY to remove it and plane the root effectively, but a few months later it may well be that there is no significant reduction in the pocket depth, because there is still inflammation there, implying still the presence of bacteria borne in residual calculus.
In this case, the periodontist will become involved. Now things have gone on too far, and the limitation of access to the calculus by the presence of the gingiva will have to be eliminated, in other words the periodontist will cut the gingiva and move it aside so he/she has direct access to the area. Then the root surfaces even close to the bone can be smoothed very well while the calculus is completely removed.
After the flap is laid open and the calculus removed and the tooth surface smoothed, the gingival tissue is sutured back again, and often a kind of plaster dressing is placed over the area while it heals.
The healing from this procedure, called OPEN debridement – the removal of calculus debris by opening the tissue – takes some period of time, and is generally rather uncomfortable. It is best to avoid this, and the way to do this, of course, is good HOME CARE.
Bottom Line for Periodontal Therapy
At HOME the best you can do is keep the plaque from accumulating around your teeth for any significant amount of time. This involves brushing and flossing and even brushing with little brushes into the space between the teeth or between the roots.
Flossing technique requires some training, but the WILL to do it is more important.
Once plaque has remained on the tooth for long enough, the bacteria within will create HARD deposits, called calculus, which CANNOT be removed by brushing and flossing.
As we have seen the calculus deposits perpetuate the periodontal disease which causes many people to lose teeth.
Removal of the calculus requires scaling and possibly root planing, and possibly surgical procedures. But, if these deposits are left in place, you are destined for continued discomfort, poor appearance, and eventually tooth loss.
It does NOT require much to maintain the oral condition in most circumstances, and NOT too much effort in the dental office to get you back on track if you have been remiss for some small period of time. That period of time is a WEEK or TWO.
Good home care habits are the most important thing, as we all know. But here the result of bad habits may be serious.